Article Text

Statistics from Altmetric.com
Description
A 42-year-old woman with a history of hypothyroidism and Addison’s disease presented with acute onset of breathlessness, chest pain and dry cough. The chest pain was pleuritic in nature and radiated into the back. On physical examination, she was hypotensive with blood pressure of 87/54 mm Hg. Her pulse rate was 95/min with normal jugular venous pressure. Respiratory system examination revealed mild tachypnoea (RR 20) without any crackles or wheezes. A chest radiograph was unremarkable. Oxygen saturations were 98% breathing 24% oxygen and arterial blood gas analysis showed pH 7.36, pO2 13.5 kPa, pCO2 4.4 kPa and HCO3 20.3 mmol/l. The white cell count was 12.3×109/l and C reactive protein 44 mg/l (normal range 0–8). Biochemical profile showed hyponatraemia and hyperkalaemia, consistent with adrenal insufficiency. An echocardiogram was unremarkable. Because there was no explanation of her dyspnoea, a CT pulmonary angiogram (CTPA) was obtained. The CTPA showed no pulmonary emboli, but demonstrated right subclavian vein stenosis with collateral circulation (figures 1 and 2). On the basis of these radiological findings, a diagnosis of right subclavian vein obstruction or thoracic inlet syndrome (TIS) was made. The patient denied neck or arm pain, numbness, or tingling. In this case, the patient’s presentation was incidental to the diagnosis of TIS and she responded well to steroid replacement for acute adrenal insufficiency on a background of Addison’s disease. Twelve months following the initial presentation our patient remained asymptomatic from TIS. TIS is characterised by compression of one or more of the neurovascular structures such as subclavian vein/artery and brachial plexus crossing the thoracic inlet. It is classified into subgroups on the basis of neurologic or vascular structures involved. The principal causes of TIS include skeletal and bone abnormalities such as a cervical rib, soft tissue abnormalities and poor posture and weak muscular support in thin women. TIS may have various clinical presentations depending upon the anatomical structures involved. More than 90% of cases present with neurological symptoms of pain, paraesthesia or weakness of upper arm or hand. As lower trunk of brachial plexus is frequently affected, TIS manifests as symptoms of C8/T1 nerve involvement with pain and paraesthesia affecting the ulnar border of forearm along with corresponding area of the hand and fingers. Vascular presentations include Raynaud’s phenomenon,1 diminished upper limb pulses with bruit over subclavian artery and cyanosis of hand on the affected side. Electrophysiological evaluation is indicated if there are neurological symptoms such as pain, paraesthesia or weakness and imaging in the form of duplex ultrasound, CT, MRI with T1 weighted sequences and conventional angiography/venography are appropriate in the presence of vascular symptoms such as pain, cyanosis and swelling of the affected extremity. The management of TIS is tailored according to the patient’s symptoms and the degree of neurological or vascular compression. Exercise and physical therapy is the recommended treatment especially in neurogenic variant. Surgical decompression is reserved for patients with symptoms of vascular TIS. Furthermore, a combination of surgery with intraoperative angioplasty is a safe and effective strategy in venous TIS and may reduce the incidence of postoperative recurrent thrombosis and need for subsequent stent placement.2 The prognosis of TIS is generally favourable and symptomatic success rates of 93% at 3 months and 73% at 5 years have been reported following surgical intervention.3 Although duplex sonography and MR imaging are invaluable for the diagnosis of vascular TIS,4 5 this case illustrates that CTPA may be of benefit for the diagnosis of this syndrome in an appropriate clinical context. Clinicians may identify similar incidental cases more frequently in view of increasing availability and use of CTPA.

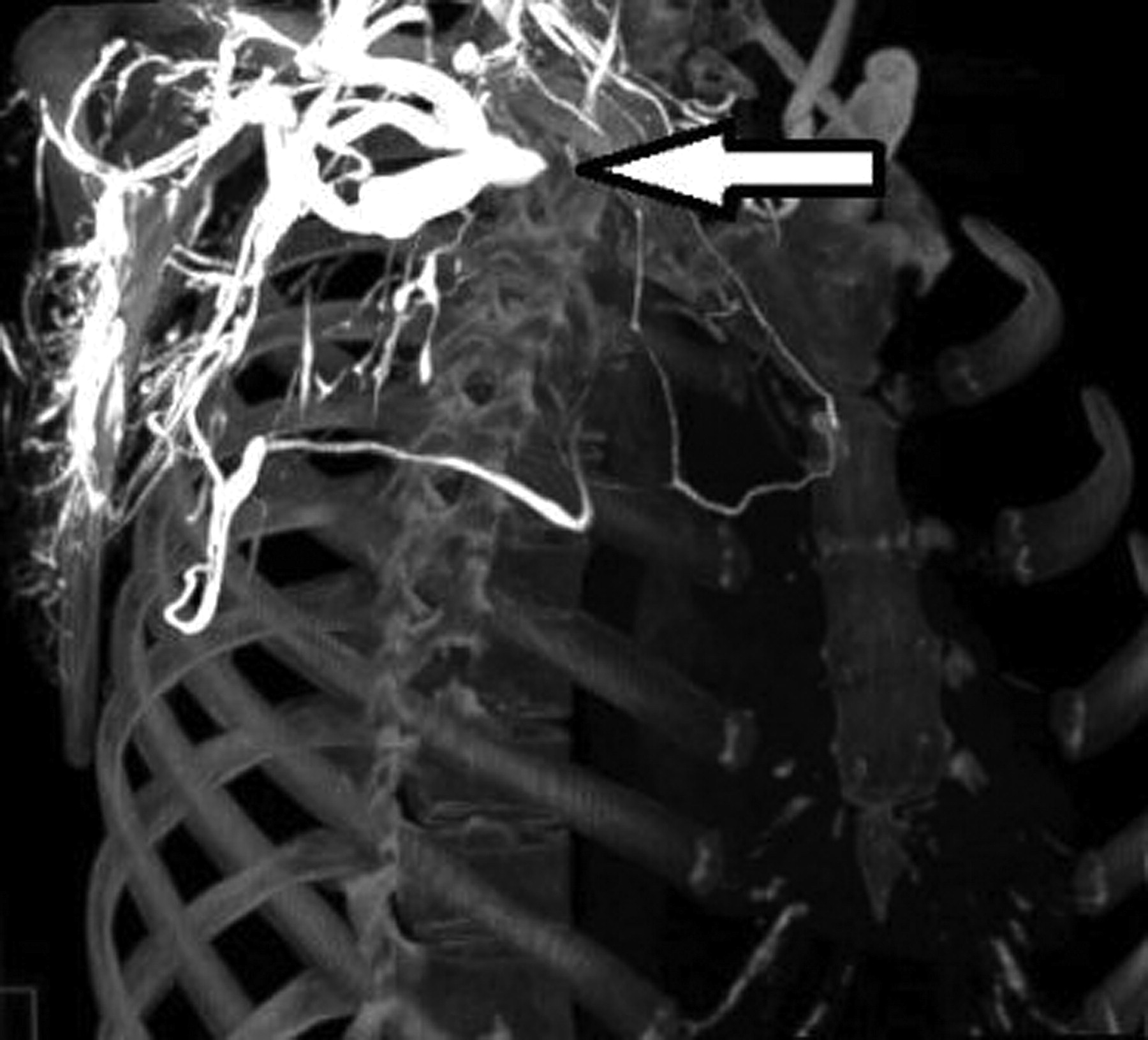
Right anterior oblique reconstruction demonstrating right subclavian vein stenosis (white arrow) and established collateral circulation.

{kind=link}
{kind=link}
Reformatted image to demonstrate the bony structures of thoracic cage. Arrow denotes subclavian vein obstruction.
Learning points
▶ Thoracic inlet syndrome (TIS) may be diagnosed by CT pulmonary angiogram.
▶ The management of TIS depends on the degree of neurological or vascular compression and the presence of associated symptoms.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.