Article Text

Statistics from Altmetric.com
Description
We are reporting a case of a 5-year-old asymptomatic boy who had grade 3 ejection systolic murmur in pulmonary area on cardiac examination. 2D echocardiography showed dilated right atrium (RA) and right ventricle (RV) suggesting increased pulmonary to systemic flow. Suprasternal echocardiographic view raised doubt of vertical vein. There was no visible atrial septic defect (ASD) or significant pulmonary arterial hypertension. Partial anomalous pulmonary venous connection (PAPVC) was suspected without an associated ASD. This pulmonary venous anomaly is extremely rare and difficult to diagnose. Clinically, PAPVC is often asymptomatic and tends to go unnoticed until adulthood, and usually diagnosed during investigation of another illness.1 Left untreated, long-standing PAPVC predisposes the patient to right-sided volume overload, tricuspid regurgitation, arrhythmias, pulmonary hypertension, irreversible pulmonary vascular disease, right ventricular dysfunction/ failure. The development of symptoms and complications from PAPVC depends on the shunt fraction and thus on the number of pulmonary veins anomalously draining to the right heart. Surgical repair is warranted in cases of significant left to right shunt. In earlier times, catheter-based angiography was the imaging modality of choice in such cases. Nowadays, this has been superseded by echocardiography, CT angiography and MRI. Trans-oesophageal echocardiography (TEE) is able to image all four pulmonary veins in most of the cases, is not a good option in small children, being an invasive procedure necessitating general anaesthesia (GA). CT/MRI scans are reliable non-invasive modalities and avoids GA required for doing a conventional angiogram/TEE in children.2 3 These imaging techniques help in correct diagnosis and play an important role in proper preoperative planning before surgery. Cardiac MRI is useful for the diagnosis of congenital heart diseases as it provides both anatomical and physiological data far superior than CT and avoids unnecessary radiation.2 Lesser availability and cost are major limitations for the use of MRI in our centre as in other developing countries. In our case, we used CT imaging because of the same reason. Our patient had a very rare type of pulmonary venous connection which was suspected after seeing RA and RV dilatation on 2D echocardiography (figure 1) and isolated upper lobar pulmonary segmental hypervascularity on chest roentgenogram, (figure 2) cause of which was confirmed by CT angiographic imaging (figures 3 and 4). Though, there is a case report mentioning isolated left pulmonary veins draining in to vertical vein diagnosed by cardiac CT,4 our case is unique in having isolated bilateral upper lobar anomalous pulmonary venous connection and normal drainage of both lower lobe pulmonary veins to left atrium. In this case, cardiac CT imaging clearly delineated the pulmonary venous anatomy further substantiating the role of non-invasive modalities. The patient was recommended surgical correction and wanted to come back at a later date for the same.

Transthoracic 2D echocardiography arrows showing dilated right atrium (RA), right ventricle (RV) and normal left atrium (LA), left ventricle (LV).

Chest x-ray arrows showing segmental hypervascularity.
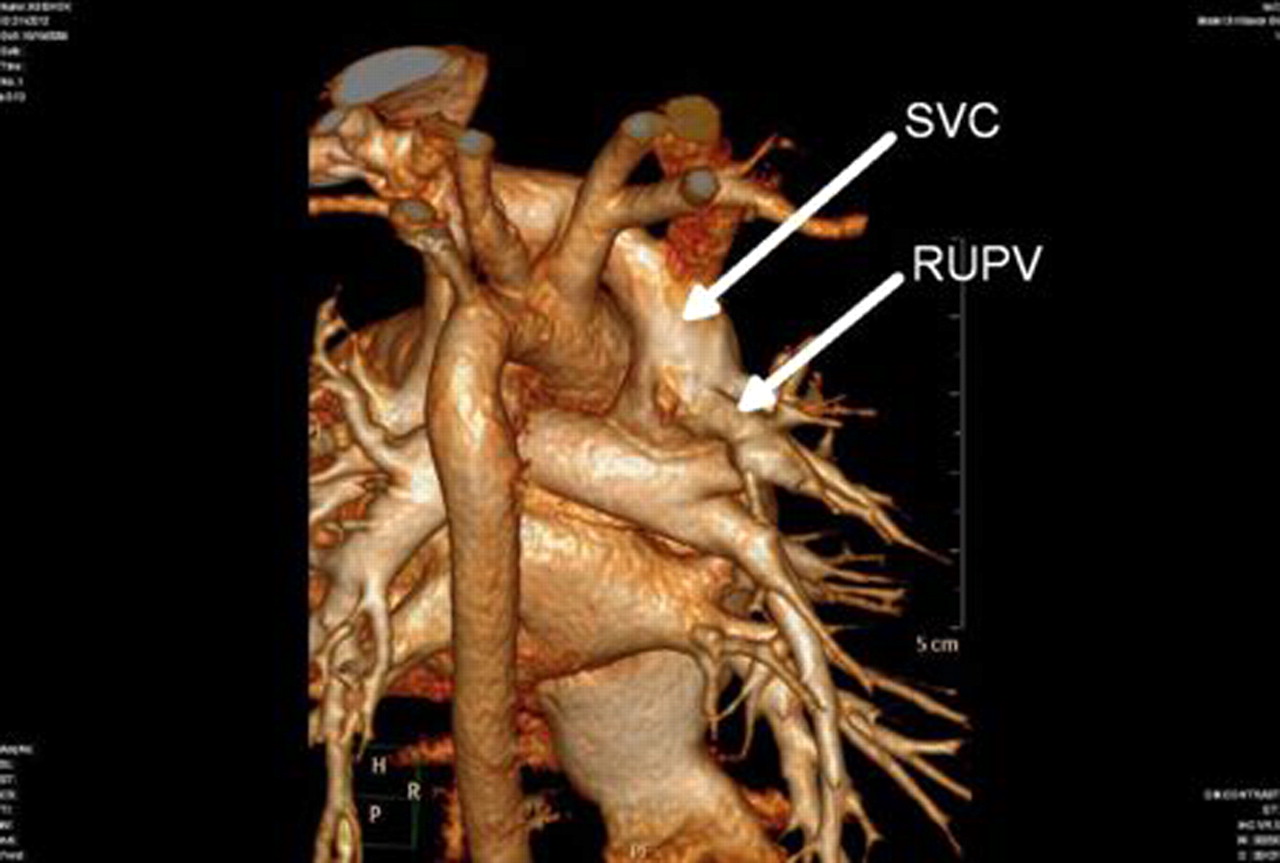
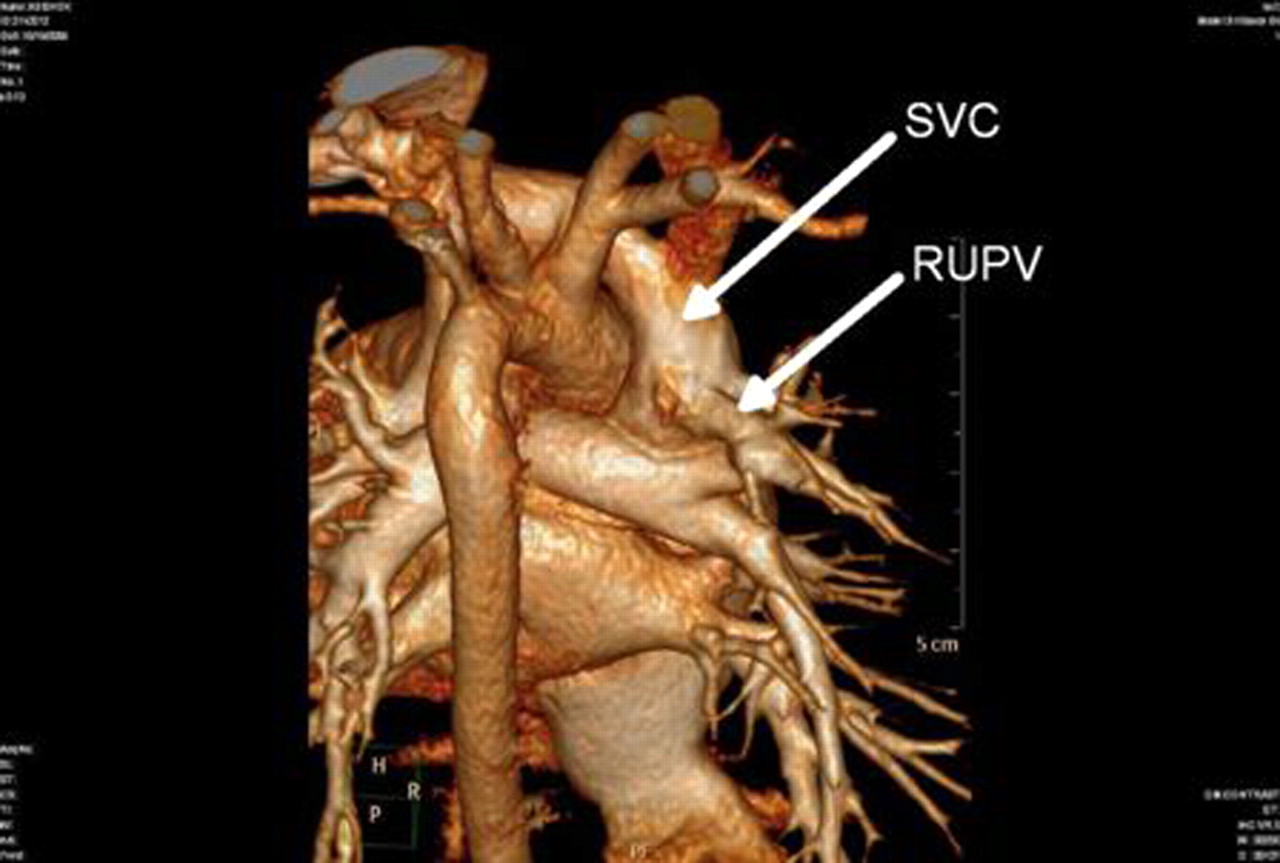
CT three dimensional imaging showing right upper pulmonary vein (RUPV) draining into right superior vena cava (SVC).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CT three dimensional imaging showing left upper pulmonary vein (LUPV) draining into vertical vein (VV).
Learning points
▶ Bilateral upper lobar PAPVC without ASD is an extremely rare congenital anomaly.
▶ Diagnosis can be easily missed and a high index of suspicion is warranted especially in cases with zonal hypervascularity on chest x-ray or unexplained RA-RV dilatation on echocardiography.
▶ CT/MRI imaging in these cases can be of paramount help in diagnosis and in proper surgical planning.
Acknowledgments
Dr G Vivek, Assistant Professor, Department of Cardiology, KMC Manipal.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.