Article Text

Statistics from Altmetric.com
Description
A man in his late thirties presented with a 6 month history of fevers, dyspnoea, productive cough and an unintentional 50 pound weight loss. Evaluation revealed cavitating Hodgkin’s lymphoma. During the hospital course, a percutaneous drain was placed into a large cavity of the left upper lobe. When the drain was later removed while the patient was undergoing mechanical ventilation, massive subcutaneous emphysema developed rapidly (figures 1 and 2A) due to a fistula at the drain site (figure 2A, red arrow). Bladder pressures rose to 26 mm Hg with concomitant decline in urine output. Abdominal compartment syndrome (defined as organ dysfunction attributable to elevated intraabdominal pressures) was diagnosed. Four incisions were made to function as pressure release ‘blowholes’ with resulting rapid reduction in bladder pressures and improved urinary outflow (figure 2B).
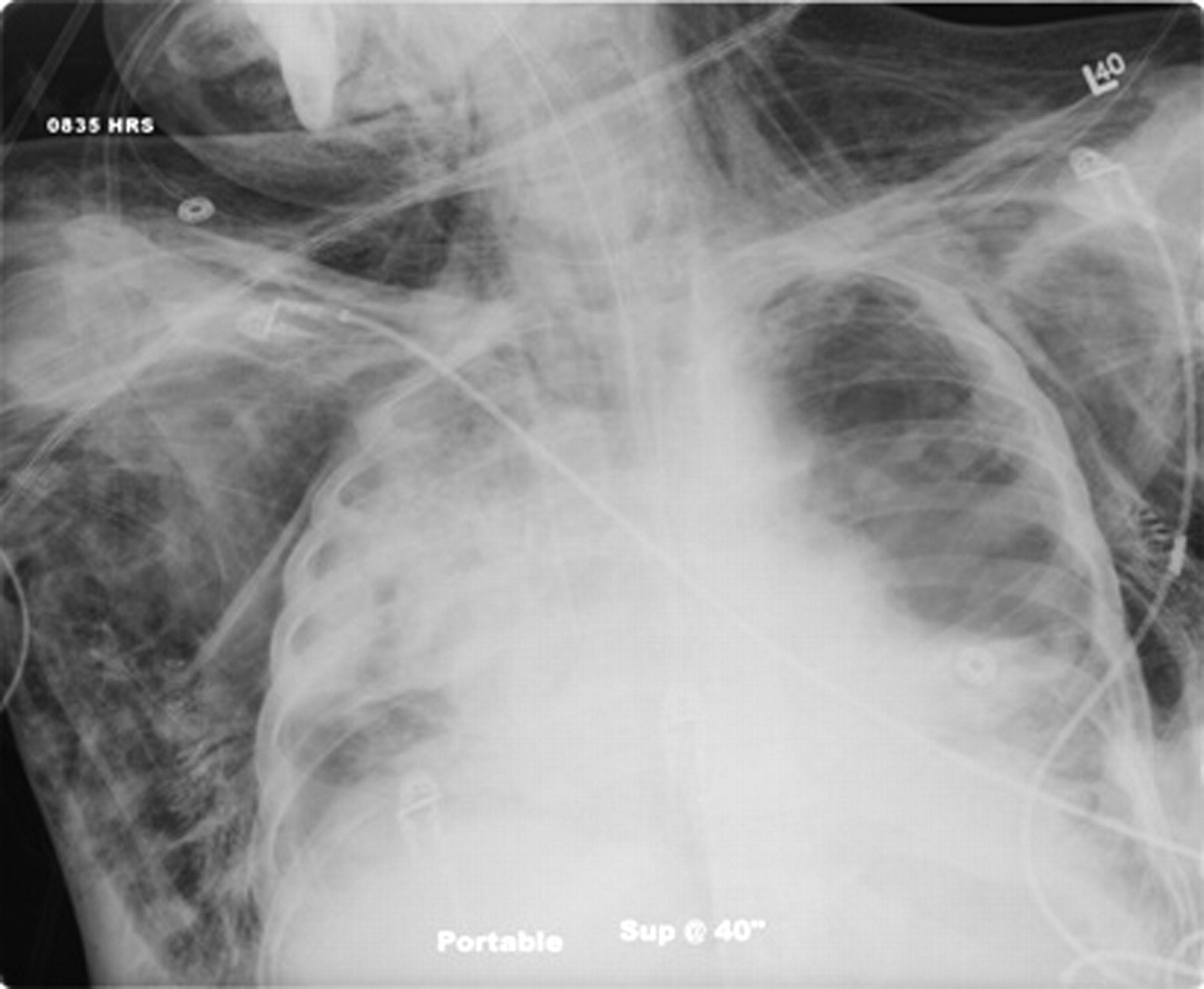
Antero-posterior radiograph demonstrating massive subcutaneous emphysema.

{kind=link}
{kind=link}
A) CT demonstrating fistula. B) Correlation of bladder pressure and urine output response to decompression of subcutaneous emphysema.
Learning points
▶ A percutaneous intrathoracic drain can lead to massive subcutaneous emphysema in a patient receiving positive pressure ventilator support.
▶ Massive subcutaneous emphysema can contribute to abdominal compartment syndrome.
▶ Decompression of massive subcutaneous emphysema can be accomplished through pressure release ‘blowholes’.
Footnotes
-
Competing interests None.
-
Patient consent Not obtained.