Article Text

Summary
The authors present a case of post endoscopic retrograde cholangio-pancreatography acute pancreatitis complicated by a pancreatico-psoas fistula, as well as reviewing similar previously published cases. The patient had a fluctuating clinical course over 4 months, developing multiple life-threatening complications including portal vein thrombosis, gastrointestinal bleeding, aspiration pneumonia and acute kidney injury on a background of chronic kidney disease. The authors followed the long-held surgical principle of draining sepsis and avoiding surgical intervention. The fistula dried up with conservative management and time also allowed portal venous collateral formation with resolution of his ascites.
Statistics from Altmetric.com
Background
Acute pancreatitis is most often a mild, self-limiting inflammatory condition but can cause multi-organ failure and death. Both acute and chronic pancreatitis can lead to pancreatic duct disruption with resultant pseudocyst formation or pancreatic ascites. Pancreatic pseudocysts can be complicated by infection, bleeding, compression of adjacent viscera, involvement of local vascular structures and fistula formation. Very rarely pancreatic secretions can track posteriorly into the retroperitoneum along the psoas muscle, and can present with an abscess or fistula in the thigh.
This case demonstrates the development of a retroperitoneal pancreatic fistula with an abscess in the right thigh, on the background of an already complex acute pancreatitis. The presented case exemplifies and highlights the need to consider important clinical challenges in diagnostic and therapeutic decision-making processes.
Case presentation
A 70-year-old man was transferred to our unit 2 weeks after developing acute necrotising pancreatitis following an endoscopic retrograde cholangio-pancreatography for choledocholithiasis. Initial cross-sectional imaging demonstrated a large complex multiloculated peri-pancreatic acute fluid collection in the lesser sac extending up into the hilum of the liver. The patient’s clinical status initially improved and the collection appeared to be resolving. He was maintaining adequate oral nutrition and hydration, and was discharged home. He re-presented with gastric outlet obstruction and tense ascites. Repeat imaging demonstrated that the complex pseudocyst remained. The portal vein was now effaced by the pseudocyst and there was associated thrombosis. There was also extensive ascites which was aspirated and sent for analysis. This was negative for amylase and had the biochemical features of a transudate. A liver biopsy was performed and demonstrated normal hepatic architecture.
Treatment
We adopted a conservative management policy including nutritional support via nasojejunal feeding and pharmacological optimisation of body fluid balance with spironolactone. A transjugular intrahepatic portosystemic shunt procedure was ruled out given the patient’s frail clinical state and impaired renal function; it was hoped that following collateral portal venous formation, the ascites would settle. After a period of 6 weeks, the patient suddenly deteriorated with a rise in temperature and inflammatory markers. Examination revealed a hot swelling in his right thigh; CT demonstrated an extensive peri-pancreatic collection, extending via the right psoas muscle into the right thigh (figures 1 and 2) with abscess formation within the thigh. This was drained percutaneously, amylase rich (1037 IU/l) pus was aspirated, confirming a diagnosis of pancreatico-psoas fistula. The drain was left in situ until dryness. Octreotide injections, 200 mcg three times daily, were administered. Following a brief improvement in the patient’s condition, he developed further sepsis secondary to infection of the pancreatic pseudocyst, which was treated with percutaneous transgastric drainage.

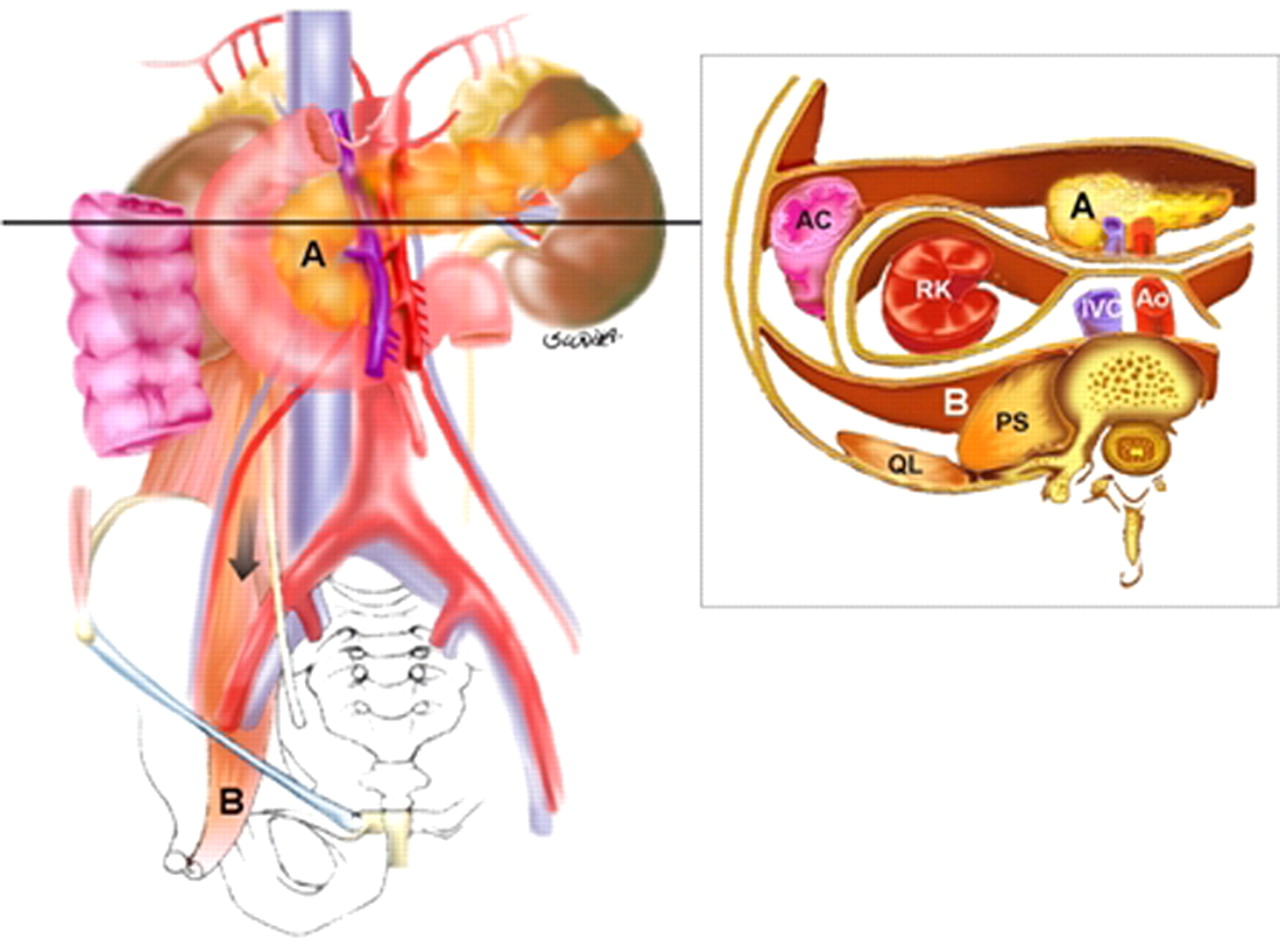
(A) demonstrates the site of the fistula as indicated by the asterisk, lateral to the femoral artery. Note the large volume ascites which on no occasion had raised amylase levels. (B) demonstrates the fistula track as indicated by the asterisk, adjacent to the psoas muscle.
{kind=link}
{kind=link}
Proteolytic fluid from a pancreatic pseduocyst can extend into the iliopsoas compartment beneath the inguinal ligament; this path of spread occurs via the inferior portion of the anterior pararenal space, which communicates freely with the posterior pararenal space.19
Outcome and follow-up
The patient had a fluctuating clinical course over 4 months during which he developed several complications including acute upper gastrointestinal bleeding secondary to a pseudoaneurysm of the left gastric artery treated by angiographic embolisation; aspiration pneumonia requiring invasive ventilation; episodes of acute kidney injury on a background of chronic kidney disease.
Through treatment of sepsis and nutritional support the patient gradually improved with resolution of the peri-pancreatic inflammation, gastric outlet obstruction, renal impairment and ascites. He was discharged home fully independent.
Discussion
Pancreatic pseudocysts complicate between 5% to 16% of patients with acute pancreatitis.1 Treatment is reserved for symptomatic cysts. The method of treatment depends upon patient factors, location of the cyst and whether there is debris within.
Acute fluid collections lacking a cyst wall arise early in the course of acute pancreatitis. Pseudocysts of the pancreas are localised fluid collections that present for more than 6 weeks, rich in pancreatic enzymes and surrounded by a wall of granulation tissue and extracellular matrix as opposed to true pancreatic cysts lined by epithelium.2 3
Initial diagnosis is usually achieved by imaging studies including transabdominal ultrasonography and CT scanning. CT offers high sensitivity rates of 82% to 100%.2 3 Endoscopic ultrasound is highly sensitive for distinguishing between different types of pancreatic cystic lesions.
The pathogenesis of pancreatic pseudocysts is related to pancreatic duct disruption with secretions typically confined to the lesser sac although they can extend cranially or caudally following anatomical planes. Pseudocysts have been reported in unusual locations including the mediastinum,4 5 pleura,6 7 liver8 and scrotum.9 Few reports have described a pancreatic pseudocyst involving the psoas muscle and inguinal region.10,–,18 In the present case, reviewing the cross sectional imaging, the pseudocyst progressively tracked into the right retroperitoneum, anterior to the psoas and into the thigh. Its presence was only discovered when the patient presented with a right thigh abscess. This was treated with percutaneous drainage and the somatostatin analogue, octreotide.
Ten previously published cases were identified in the English language literature and were reviewed (table 1).10,–,18 Eight patients presented with a painful groin mass and two with hip pain. Only two cases followed a recent episode of acute severe pancreatitis with the remainder complicating chronic pancreatitis. Six cases were treated by percutaneous drainage, and the remainder with a variety of surgical interventions, of which two were for fluid collections masquerading as incarcerated inguinal herniae.
In general, decisions regarding intervention in complicated or symptomatic cases require multi-disciplinary input. We adopt a step-up approach starting with internal or external percutaneous drainage. If fistula output fails to resolve, endoscopic insertion of a pancreatic duct stent is attempted. In managing cases of complex pancreatico-pleural fistula in our unit, pancreatic duct stenting has been successful in treating cases refractory to percutaneous drainage.6 Open surgical intervention is ideally avoided due to additional inflammatory burden, and higher morbidity and mortality compared with endoscopic and minimally invasive therapeutic drainage techniques.2
Learning points
▶ Pancreatitis is commonly complicated by pancreatic pseudocysts which can result in fistula formation.
▶ In the pathogenesis of pancreatic pseudocysts, secretions may extend to unusual anatomical locations, presenting with clinical features which may be misinterpreted unless there is a high index of clinical suspicion.
▶ CT is routinely the diagnostic imaging modality of choice for pancreatic pseudocysts.
▶ Management of pancreatic pseudocysts varies with the patient’s clinical condition and local expertise, requiring multi-disciplinary input.
Acknowledgments
Dr Maria Sheridan, Consultant Radiologist, St James’ University Hospital, Leeds Teaching Hospitals NHS Trust
References
Footnotes
-
Competing interests None.
-
Patient consent Not obtained.
Linked Articles
- CORRECTION