Article Text

Summary
Spillage of gallstones in the peritoneal cavity during laparoscopic cholecystectomy (LC) occurs at rates varying from 5.7% to 16%. These gallstones often cannot be retrieved and can cause early and late abscesses at rates ranging from 0.08% to 1.4%. The case of an 86-year-old woman with colon cancer is described because during an elective right hemicolectomy a granuloma of the omentum with retained gallstones from LC performed 8 years earlier was unexpectedly found. Importantly, the gallstones were found high up in the abdominal cavity. Moreover, this report reaffirms the excellent response of the peritoneal cavity defence mechanisms for protecting patients against gallstones through asymptomatic omental granuloma. Current data indicate that every effort should be made to retrieve spilled gallstones, but routine conversion to an open cholecystectomy is not recommended. Identifying factors that impair host defence mechanisms should help surgeons’ decision-making.
Statistics from Altmetric.com
Background
The cholecystectomy rate in European countries in 1999 was approximately 100 per 100 000,1 while 600 000 cholecystectomies were performed in 1991 in the USA with an estimated 80% performed laparoscopically.2 Laparoscopic cholecystectomy (LC) is a safe and effective procedure for the management of gallstone cholecystitis.3,–,5 LC is associated with decreased postoperative pain, shorter hospitalisation, a faster return to regular activities and better cosmetic results than open cholecystectomy and has become the preferred method for surgeons and patients.
Nevertheless, serious LC complications such as bile duct (0.6%), bowel (0.14%) and vascular (0.25%) injuries may occur.3
Intraoperative gallbladder perforation and spillage of bile and gallstones into the peritoneal cavity commonly occur but are rarely associated with increased morbidity. It is obvious that the defence mechanisms of the peritoneal cavity are capable of protecting the patient from the retained gallstones in the vast majority of cases. The fate of retained gallstones in the asymptomatic patient is largely unknown.
On the other hand, any failure of the defence mechanisms will result in adverse consequences, the most common of which are surgical site infections (SSI). Identification of those at high risk for SSI from retained gallstones may help to select patients for conversion to an open cholecystectomy.
This review focuses on the high abdominal location in which gallstones retained following LC were found, the manner in which they were isolated by the peritoneal defence mechanisms, and clinical management decisions.
Case presentation
An 86-year-old woman with chronic iron deficiency anaemia due to a carcinoma of the hepatic flexure was admitted for elective surgical resection.
Her medical history included long-standing arterial hypertension, a hysterectomy 15 years earlier, pericarditis 10 years earlier, LC 8 years earlier and total right knee replacement 3 years before admission.
Investigations
On admission, haemoglobin was 9.7 g/dl and serum albumin 2.8 g/dl, but the remaining routine liver and renal function biochemistry tests were normal.
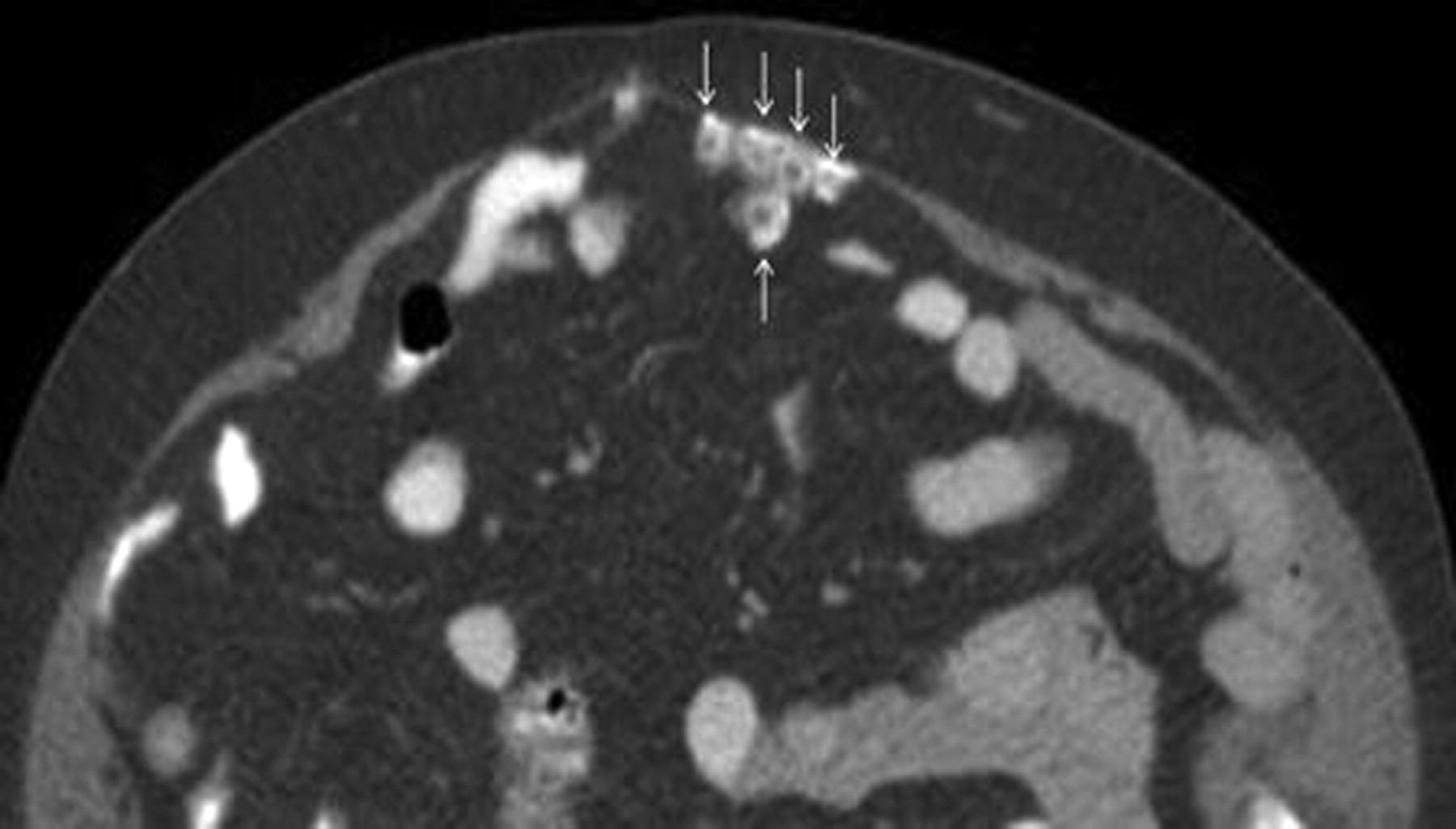
Colonoscopy and biopsy had confirmed the presence of adenocarcinoma in the hepatic flexure; CT scan indicated no liver or other distal metastases. Retained gallstones from the previous LC were visible but not reported (figures 1–3).

Abdominal CT scan showing gallstones embedded in the omentum (arrows). All gallstones had a marked peripheral opacity with central lucency.

Abdominal CT scan showing a gallstone (arrows) in the pelvis.

Abdominal CT scan showing the gallstone (arrows) lying in the pelvis just above the peritoneal reflection.
Differential diagnosis
No diagnostic dilemmas were encountered during treatment of the patient. Surgeons and radiologists were not aware of the history of retained gallstones from the previous LC.
Treatment
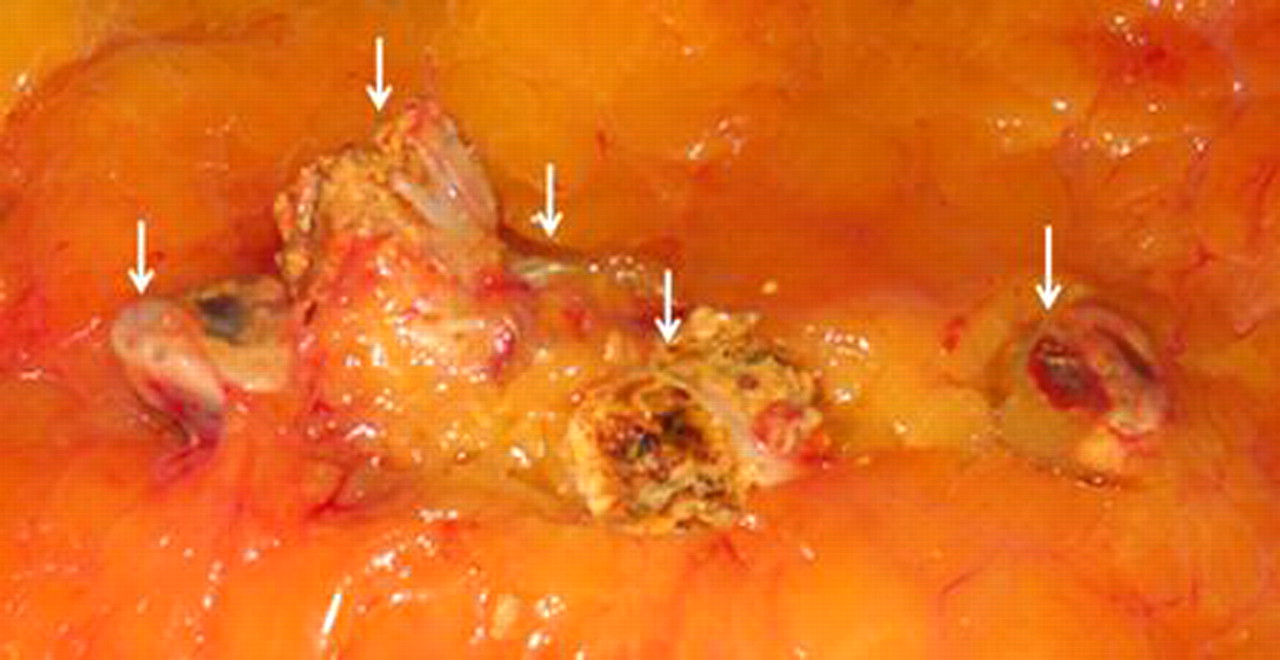
The patient underwent an elective laparotomy where intraoperative inspection and palpation confirmed the existence of the colonic tumour. Unexpectedly, a thickening of the greater omentum was noted distant from the tumour and close to the omental free edge, which corresponded to the middle of the transverse colon. This portion of the omentum was resected and gallstones trapped in the omentum were identified (figures 4 and 5). No local factors such as adhesions or the colonic tumour could explain the high location in which these gallstones were retained. Further palpation revealed one more gallstone loosely attached in the pelvic peritoneum which was retrieved. A typical right hemicolectomy was performed, recovery was uneventful and the patient was discharged after 7 days.

Resected omentum with the embedded gallstones (arrows).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Partially dissected omentum (shown in figure 4) showing gallstones (arrows).
Outcome and follow-up
Histopathology confirmed the diagnosis of a colonic adenocarcinoma staged as T3N0M0. Microscopic examination of the resected omentum revealed a foreign body type granuloma consisting of mature fatty tissue with focal fat necrosis, fibrosis and calcification surrounding the gallstones without evidence of metastasis from the colonic adenocarcinoma. The patient has remained well over the last 6 months.
Discussion
The patient initially underwent a laparotomy because of the colon cancer and even retrospectively no symptoms could be attributed to the retained gallstones in the abdomen following LC 8 years earlier.
Most perforations of the gallbladder occur either during its dissection from the liver bed (47%), during its extraction through the abdominal wall (21%) or are the result of intraoperative retraction (14%).6 Bile and gallstone spillage also occurs during intraoperative cholangiography. It seems that the retained gallstones in our patient were spilled during gallbladder extraction through the abdominal wall because their location in the greater omentum corresponded to the umbilical port of the LC.
The gallstones were found high up in the abdominal cavity in a supine individual, where they were trapped by the expected inflammatory response of the omentum, although gravity had caused one of the gallstones to descend into the pelvis.
Frequency of gallstone spillage
Intraoperative perforation of the gallbladder with spillage of bile and/or gallstones into the peritoneal cavity occurred in 29% of 1059 consecutive LC,6 while the reported rates of gallstone spillage only were 5.7% in 10 1747 and 16% in 856 patients.8 Increasing age, body weight and the presence of omental adhesions were found to be significant factors predisposing to intraoperative perforation of the gallbladder.6
Complications of retained gallstones
Perioperative death rates attributed to retained gallstones are unknown but probably low. No perioperative deaths were attributed to retained gallstones in three large series.6,–,8
Although rarely, retained gallstones in the abdominal cavity following LC can cause a variety of complications, some of which are harmful.8 Postoperative pyrexia occurs significantly more often in patients who experience gallbladder perforation during LC than in patients who do not.6 Most of the reported complications are infections, although small bowel obstruction9 10 attributed to a localised intense inflammatory reaction to gallstones has been reported.
Intra-abdominal abscess formation occurred at a rate of 1.4%6 during the mean 3.3 years (range 2.1–5 years) of follow-up in a series of patients with bile (177) and gallstone (103) spillage after LC. Another study showed that among 547 patients with spilled and retained gallstones, eight (0.08%)7 developed an abscess postoperatively that required reoperation.
Locations of abscesses
The most common of locations for abdominal abscesses8 attributed to gallstone are the perihepatic region, Morrison’s pouch, right flank, peritoneal-cutaneous sinus,11 right upper quadrant, right lower quadrant, pelvis and umbilicus.12 More rarely, infections attributed to gallstone migration may occur in the abdominal wall,11 the pleura and the lung.6 13
The inflammatory response of the omentum trapped the gallstones of our patient in a high position. Gravity, low subdiaphragmatic abdominal pressure, anatomical factors as well as pneumoperitoneum result in the migration of gallstones into obscure tissue planes of the abdominal cavity making detection and retrieval of all spilled gallstones during LC difficult or impossible. Consequently, the dilemma of converting LC into an open procedure in order to remove spilled gallstones often arises. Hence, reasoned clinical decision making remains important.
CT scan
The gallstones were visible in a postoperative CT scan of the described patient. Known retained gallstones in the abdominal cavity were documented by CT scan in only two of 22 asymptomatic patients.14 The gallstones were visible in the preoperative CT scan of the described patient.
Management
Conversion to an open cholecystectomy is not indicated following gallstone spillage. During the early laparoscopic years, a rate of 5.8% of conversion to an open cholecystectomy for gallstone retrieval was documented for some surgeons.7 A reoperation rate of 3% (eight patients) during the early postoperative period was reported in a group of patients with perforated gallbladder during LC, of whom three required open drainage of an intra-abdominal abscess.6 Currently, routine conversion of LC to the open approach for gallstone retrieval is not recommended6,–,8 since the reported incidence of subsequent abscess formation is low (less than 5%).12
Some authors suggest conversion of LC to an open cholecystectomy when a large number of gallstones cannot be retrieved laparoscopically and the bile contains bacteria.8 Supporting this view is the reported ineffectiveness of percutaneous drainage of intra-abdominal abscesses because the gallstones are not removed6 12 and surgery is then required to remove them.
Successful percutaneous removal of retained gallstones has been reported, but there are limitations regarding size of the stones and the area in which they are located.15
Antibiotics
A single intravenous dose of prophylactic antibiotic8 in the immediate preoperative period or one preoperative and one postoperative antibiotic dose is good practice for elective cholecystectomies.6
Evidence-based guidelines recommend that patients undergoing cholecystectomy for acute cholecystitis should have antimicrobial therapy discontinued within 24 h unless there is evidence of infection outside the wall of the gallbladder.16 Antibiotics for a longer time were recommended by some authors17 and were administered orally for 5 days to patients with gallstones retained in the abdominal cavity following LC by other authors.14 However, the potential benefit from postoperative administration of antibiotics for more than 24 h for spilled gallstones needs further evaluation. Routine culture of bile is recommended because it can help the selection of appropriate antibiotics if the need arises.
Is routine follow-up required?
Experimental data indicate that a 90-day follow-up may be too short for the meaningful determination of the long-term effects of gallstones retained in the abdomen.18 Long-term follow-up of asymptomatic patients with retained gallstones does not seem to prevent long-term complications.14
Peritoneal defence mechanisms against gallstones
The rational and empirical approach of not converting LC to an open procedure for gallstone retrieval is based on clinical data and long-term clinical results following the spilling of bile and gallstones.
However, the status of the immune defence mechanisms of patients is not routinely explored. This lack of preoperatively identifying patients at risk of infectious complications deserves further consideration. The determinant factors of any infectious process can be classified into three groups19: (1) factors affecting the local defence mechanisms (eg, surgical trauma, presence of gallstones); (2) the bacteria (inoculum, virulence); and (3) the systemic host defence mechanisms. This biological model applies to the infectious complications caused by retained gallstones.
Gallstones
Gallstones in the abdomen cause a local inflammatory response and adhesions.20 They may be trapped by the omentum as has been previously shown in rats20 as well as in humans.21
The omentum is a primary peritoneal defence organ.22 Of particular importance are islands of omentum containing accumulations of immune cells around the capillaries called ‘milky spots’.23 24 Injury and foreign bodies activate the omentum and lead to an expansion of the ‘milky spot’ areas and increase its growth, angiogenesis, chemotactic factors and progenitor cells, all of which promote healing and regeneration of the injured tissues.23
Granuloma
Relatively inert foreign bodies that cannot be phagocytosed by single macrophages stimulate the formation of foreign body granulomas. A granuloma represents a focal chronic inflammatory response consisting of aggregation of macrophages, lymphocytes, epithelioid giant cells and occasionally plasma cells. Fibroblasts and connective tissue surrounding the foreign bodies develop into long-standing granulomas.25 In the patient presented here, excellent omental properties isolated the gallstones by forming an asymptomatic granuloma. Foreign body granuloma formation due to the spillage of gallstones has been documented in other clinical studies.21 26 27 The host defence mechanisms of the peritoneal cavity keep the vast majority of patients with retained gallstones asymptomatic. However, the natural history of the pertinent peritoneal defence mechanisms remains an interesting subject for further research.
Bacteria
Bacteria were cultured in the bile of 22.2% of patients with symptomatic gallstones and in 46.1% of patients with acute cholecystitis.28 Bacteria comprise a significant portion of the substance of gallstones. Bacterial microcolonies were found in the interior of pigmented gallstones. They also adhere to the surface of gallstones, forming glycocalyx biofilms29 30 that protect them from the host defence mechanisms and antibiotics. Hence, gallstones are a sanctuary for bacteria and the nidus of abdominal abscess formation.
Experimental data also indicate that a combination of factors such as bile and gallstones in the peritoneal cavity of rats, was associated with increased intra-abdominal formation of adhesions and abscesses.20
Further understanding of the complexity and the interactions between pathogens and host defence mechanisms31,–,34 may help to select patients for conversion of LC to open cholecystectomies or additional therapies.
Learning points
▶ An excellent response of the peritoneal cavity defence mechanisms in isolating gallstones by asymptomatic omental granulomas is documented.
▶ This review reaffirms that the defence mechanisms of the peritoneal cavity are capable of protecting the patient against the vast majority of gallstones retained after laparoscopic cholecystectomy.
▶ Current data have documented that retained gallstones carry a low risk for both early and late postoperative complications (mainly abscesses), but that conversion to an open cholecystectomy is not indicated.
▶ Preoperative identification of patients at high risk for infectious complications should further optimise surgeons’ decision making and clinical outcomes.
References
Footnotes
-
Competing interests None.
-
Patient consent Obtained.