Article Text

Statistics from Altmetric.com
Description
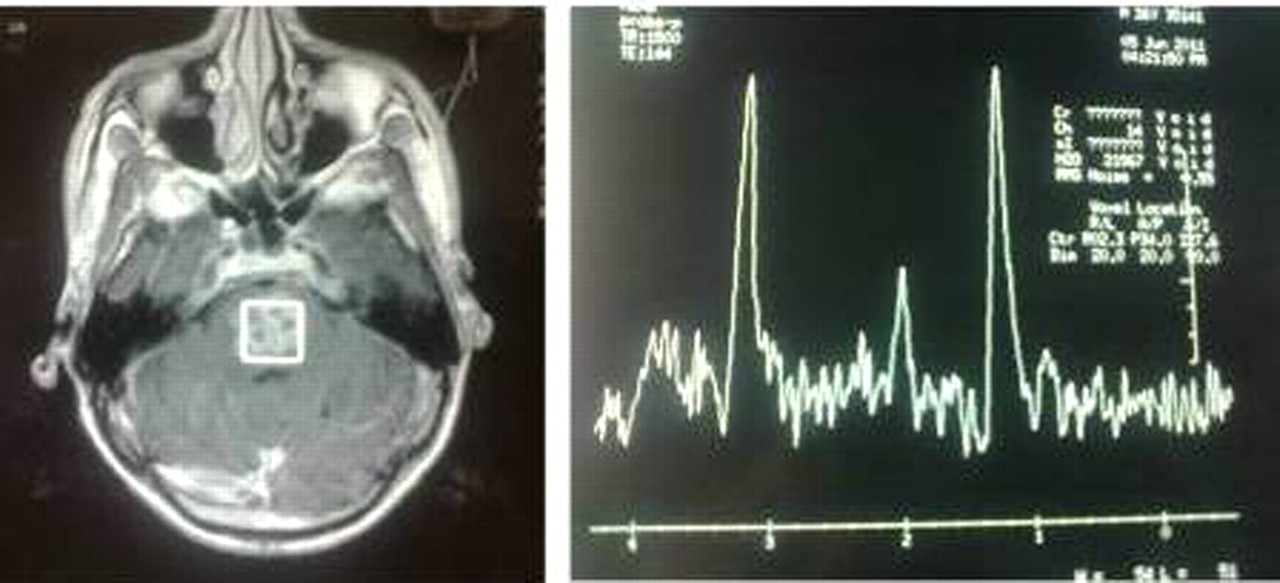
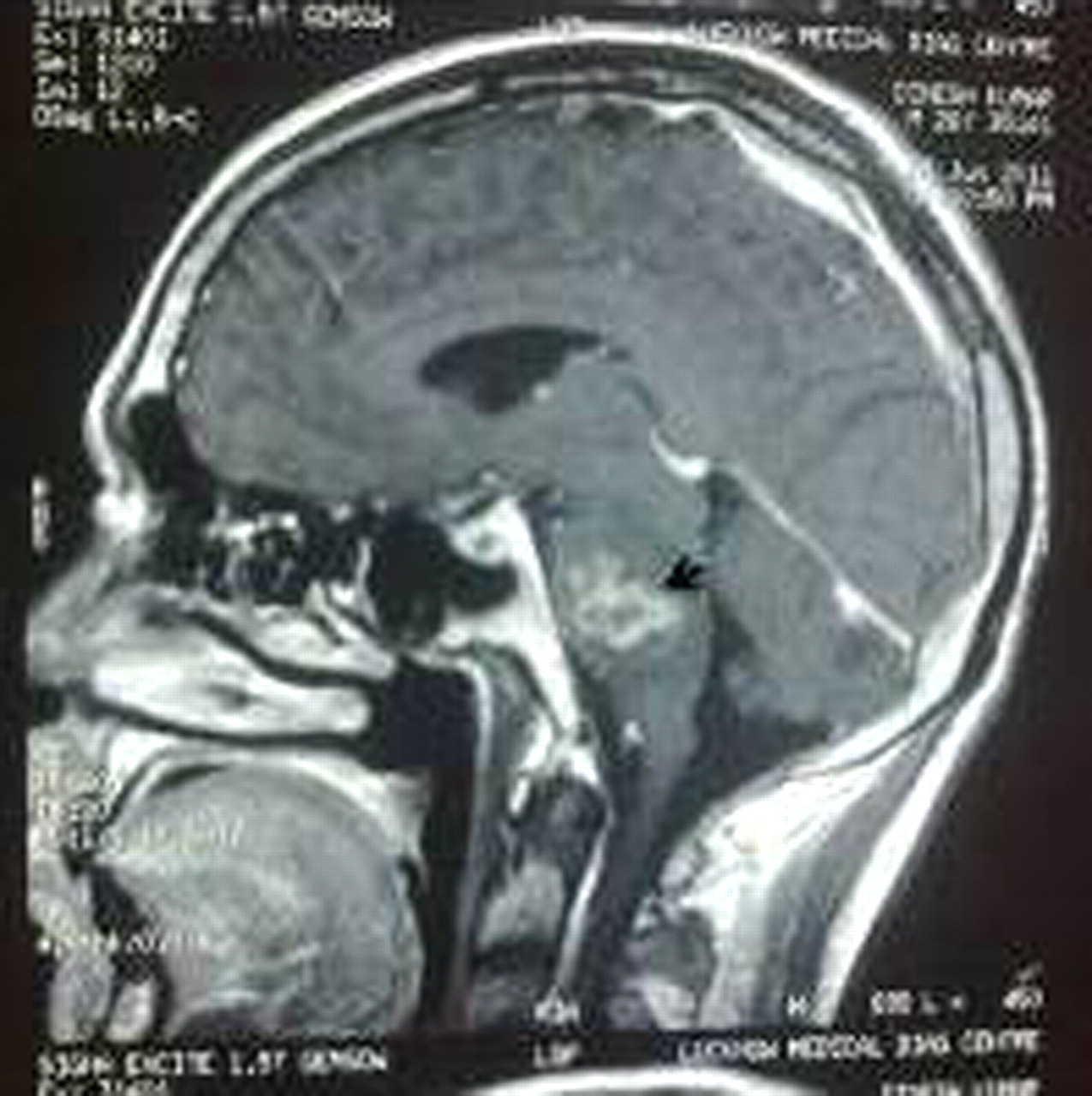
A 26 year-old-man developed progressive weakness of all limbs, hoarseness of voice and dysphagia over a period of 10 days. The patient was conscious, oriented and vital parameters were within normal limits. Neurological examination revealed; horizontal and torsional nystagmus, bilateral 9th and 10th cranial nerve involved, 3/5 muscle power in all limbs and sensory system was intact. MRI brain showed multiple small conglomerated ring enhancing lesions displaying hyperintense core on T2 weighted images (WIs) and hypointense on T1WIs and fluid attenuated inversion recovery (FLAIR) and rim was isointense to hyperintense on FLAIR and hypointense on T2WIs seen in pons (figure 1). MR spectroscopy (MRS) at the site of lesions showed increased lipid peak, decreased N-acetylaspartate peak with increased Ch/Cr ratio (figure 2).1 A tubercular aetiology was further supported by positive cerebrospinal fluid PCR for Mycobacterium tuberculosis. A diagnosis of brain stem tuberculoma was considered. Antituberculous treatment and corticosteroids were started and after 2 weeks, he became able to walk with support (muscle power 4/5), hoarseness and dysphagia also decreased. At follow-up after 1 month, he regained complete muscle power, dysphagia resolved but bit hoarseness persisted. He recuperated completely by the end of 3rd month. MRI study has been used in the diagnosis of tuberculoma in the brain, brainstem2 and spinal cord, but MRI features of tuberculosis (TB) abscesses are non-specific and may mimic abscesses of other infectious aetiology. MRS may increase specificity of diagnosis by identifying lipids within the lesions that are considered characteristic for TB. Invivo and invitro MRS has shown elevated lipid peaks within the TB lesions.3 Gliomas, metastases, abscesses and demyelinating disease were the differential diagnosis that was considered in our patient. Considering MRS to differentiate the above lesions can be helpful but clearly impracticable in all circumstances even at tertiary centres. Here MRS study safely avoided the need of brain biopsy to confirm the nature of lesion.

MRI saggital view shows multiple conglomerated ring enhancing lesions (arrow) in pons displaying hypointense core on T1W with perilesional oedema.
{kind=link}
{kind=link}
MR spectroscopy at the site of lesion shows increased lipid peak and decreased N-acetylaspartate peak with increased Ch/Cr ratio.
Learning points
▶ MRS may prove a useful non-invasive investigational tool to differentiate the lesions which are often confused with the inflammatory granulomas.
▶ The isolated occurrence of pontine tuberculoma is rarely seen. It should be kept as differential diagnosis when patients present with brainstem syndromes, particularly in the areas where tuberculosis is prevalent.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.