Article Text

Statistics from Altmetric.com
Description
A 45-year-old male, a known case of rheumatic heart disease (RHD), presented with New York Heart Association (NYHA) class III breathlessness of 6 months duration. There was no history of tuberculosis, diabetes mellitus or chronic kidney disease. A transthoracic echocardiogram showed severe mitral stenosis with an orifice area of 0.9 cm2 and a valve gradient of 23/16 mm Hg. The Wilkins score was 9 (leaflet mobility 3, valvular thickening 3, subvalvular fusion 2 and calcification 1). Percutaneous transluminal mitral commissurotomy (PTMC) was planned. Fluoroscopy of the chest in the anteroposterior view revealed atrio-ventricular (AV) groove calcification, resembling a ‘necklace’ (figure 1). PTMC was performed successfully (figure 2) and the patient is in NYHA class I at 6 months follow-up. The most common site of calcium deposits in RHD are the valve leaflets. Sometimes this extends to involve the valve ring. AV groove calcification in RHD, as seen in our case, is an extremely rare occurrence. It is possible that it represents a degenerative, calcific process of RHD which extends beyond the endocardium to involve the AV groove. The clinical presentation in the present report was due to severe mitral stenosis. Long-term follow-up is essential, as the physiological consequences of calcification in non-valvar sites are uncertain. There is a lack of data regarding the possibility of the development of constrictive physiology. However, AV groove constriction is possible, considering the site of calcification. Such cases usually present with progressive breathlessness on exertion, with a mid-diastolic murmur at the apex, simulating mitral stenosis. Therefore, in RHD, if there is a progressive worsening of cardiovascular disability, constrictive physiology secondary to AV groove calcification should be considered in the differential diagnosis. Identification of similar patients and long-term follow-up will shed light on the possible association. The Wilkins scoring system involves leaflet rigidity, leaflet thickening, valvular calcification and subvalvular disease. AV groove calcification is not included and the score remains unaffected. The main aim of PTMC is commissural separation for symptomatic relief. There appears to be no risk for haemopericardium in the presence of AV groove calcification. The consequences of balloon oversizing and inflation are valve tear and severe mitral regurgitation rather than haemopericardium.
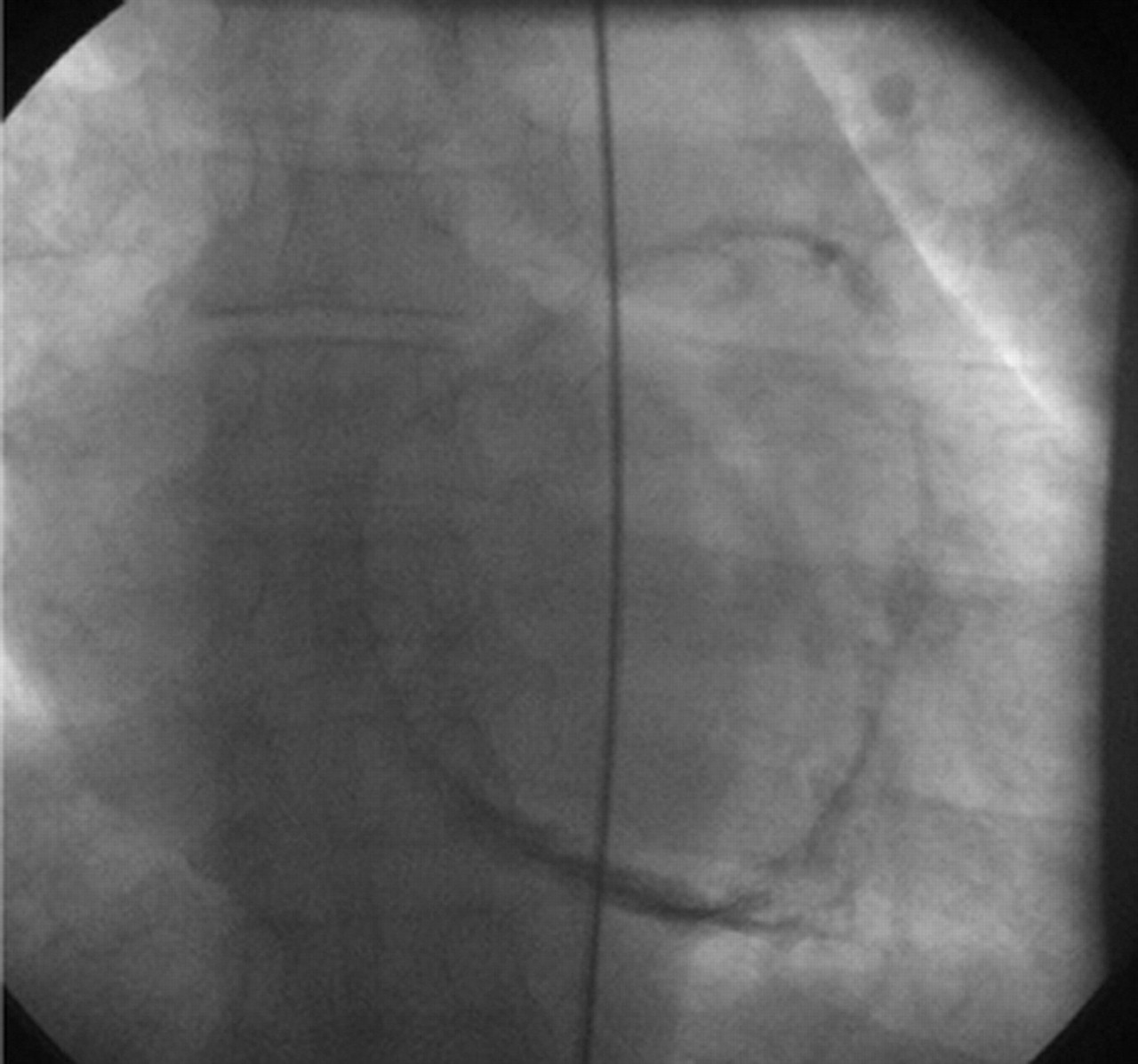
Fluoroscopy in anteroposterior view depicting atrio-ventricular groove calcification, resembling a necklace.
{kind=link}
{kind=link}
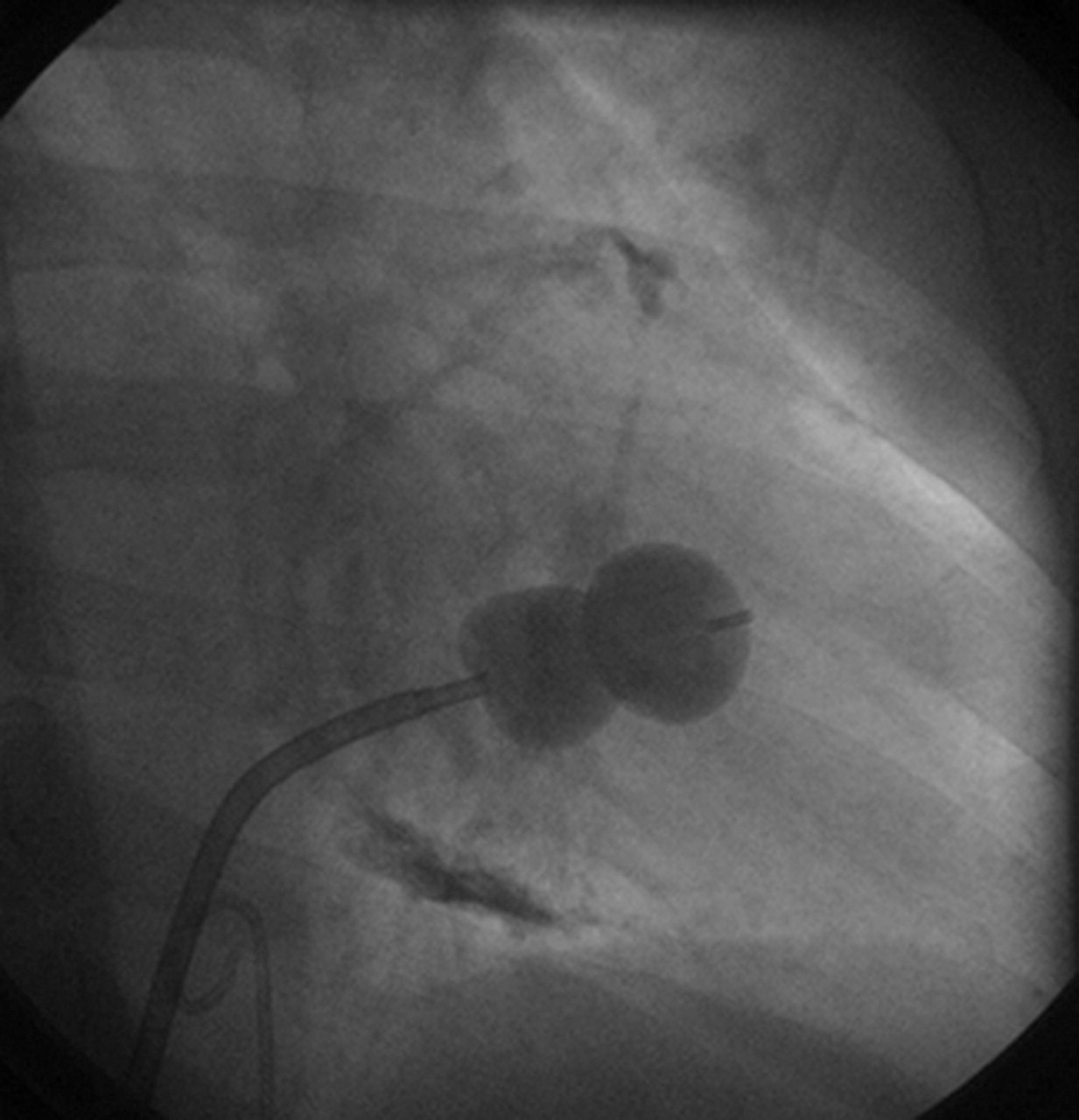
Fluoroscopy depicting the percutaneous transluminal mitral commissurotomy balloon across the mitral valve being inflated. In addition, atrio-ventricular groove calcification can be appreciated.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.