Article Text

Statistics from Altmetric.com
Description
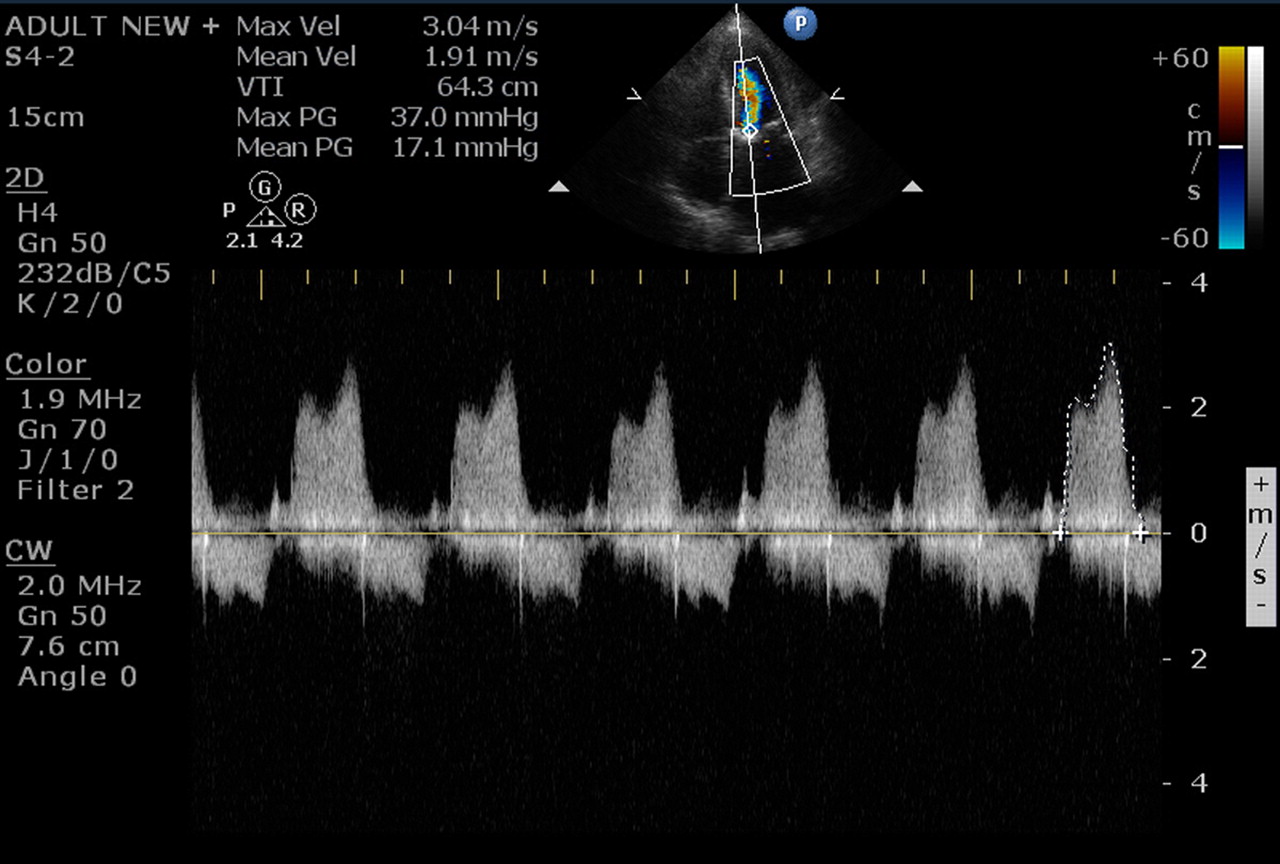
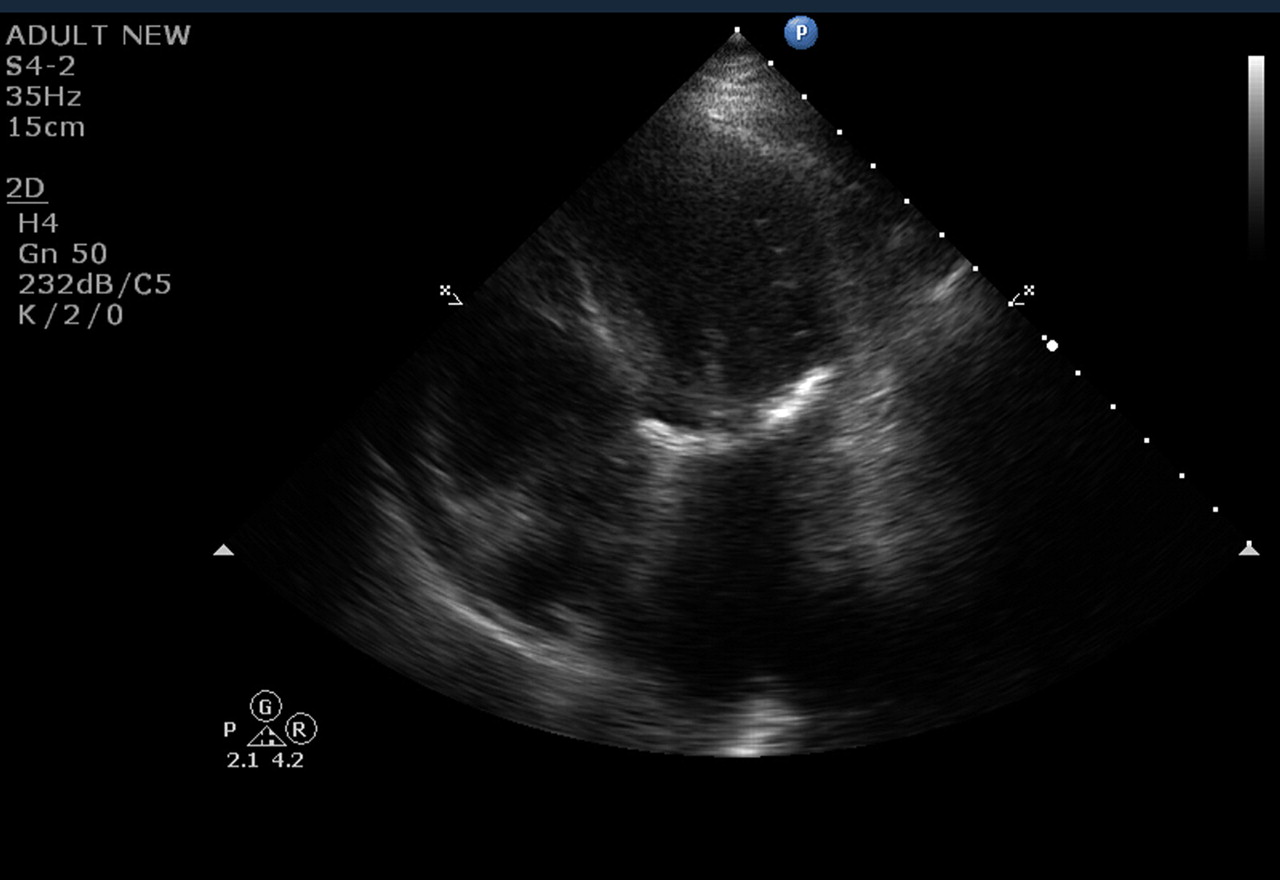
A 82-year-old woman with sedentary lifestyle presented with New York Heart Association Class IV dyspnoea and orthopnoea of 1 day duration. Clinical examination was unremarkable except for bilateral basal crepitations. There was no murmur on auscultation. Her baseline investigations including blood sugar, urea, creatinine and calcium were normal. Chest x-ray showed pulmonary venous hypertension. Echocardiogram revealed extensive calcification of mitral annulus which caused severe left ventricular (LV) inflow obstruction with gradient of 37/17 mm Hg (figure 1A,B; video 1). In contrast to rheumatic mitral stenosis, the valve leaflets were of normal thickness and had normal mobility. Degenerative mitral annular calcification is not an uncommon finding in older patients. Rarely, it may lead to significant LV inflow obstruction with pulmonary oedema.1 Mitral annular calcification should be included in the differential diagnosis of pulmonary oedema in geriatric patients. She was treated with diuretics and β blockers which provided good relief. Patient’s symptomatic class will be reassessed on optimal medical therapy and will be considered for cardiac catheterisation followed by mitral valve replacement, if symptoms do not improve with medical therapy. Mitral annular calcification results from a degenerative process in the fibrous skeleton which is probably accelerated by advanced age, hypertension, hypercholesterolaemia, diabetes mellitus and chronic renal failure. Fibrillar alteration of the collagen ultrastructure acts as a nidus for lipid deposition and the subsequent development of small foci of calcification within annulus and at points of interdigitation with ventricular muscle fibres.2 The treatment of choice is surgical excision of calcification with valve replacement or repair, if possible. The calcium bar is removed by sharp en bloc dissection followed by annular reconstruction with a strip of untreated autologous or glutaraldehyde-preserved bovine pericardium. Technically both these steps are demanding and lead to significant morbidity and mortality. In the largest published surgical series for mitral annular calcification the operative mortality was 9.3% compared with 1.5% in those without calcification.3 Nevertheless, operated patients have better quality of life with better survival rates.

Apical 4-chamber view showing dense calcification of the mitral annulus. Note the thin freely mobile valve leaflets.
{kind=link}
{kind=link}
Continuous Doppler across mitral valve demonstrating significant left ventricular inflow obstruction.
Apical 4-chamber view showing dense calcification of the mitral annulus. Note the thin freely mobile valve leaflets.
Learning points
Mitral annular calcification is not an uncommon cause of LV inflow obstruction.
Acute pulmonary oedema may be the first and only manifestation.
Echocardiogram is confirmatory.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.