Article Text

Statistics from Altmetric.com
Description
A 38-year-old patient presented with recurrent presyncope, extreme fatigue, facial oedema and weight loss. Physical examination revealed a palpable painless mass in the left supraclavicular region, facial oedema and a mild meso-systolic murmur audible at the right sternal border.
An echocardiogram revealed a mass anterior to the heart compressing cardiac chambers and the aortic root. The compression resulted in a right ventricle outflow tract (RVOT) with less than half its normal antero-posterior diameter and a fusiformly shaped left atrium (LA) of extremely reduced antero-posterior diameter as it was being compressed by the displaced aortic root. Acceleration of blood flow in the RVOT and LA was evident with colour flow Doppler imaging. The lower radial/longitudinal strain of basal-medium segments of anterior and lateral left ventricular walls was documented. A thoracic CT revealed a voluminous mass in the anterior mediastinum and a biopsy diagnosed a non-Hodgkin's lymphoma (diffuse large B cell type). Figures 1–3 illustrate cardiac involvement by the mediastinal mass.

Paraesternal long-axis view revealing direct compression of the right ventricular outflow tract by the extracardiac mass and indirect compression of the left atrium by the displaced aortic root.

Colour flow Doppler imaging unveiling acceleration of flow in the fusiformly shaped compressed left atrium.

{kind=link}
{kind=link}
{kind=link}
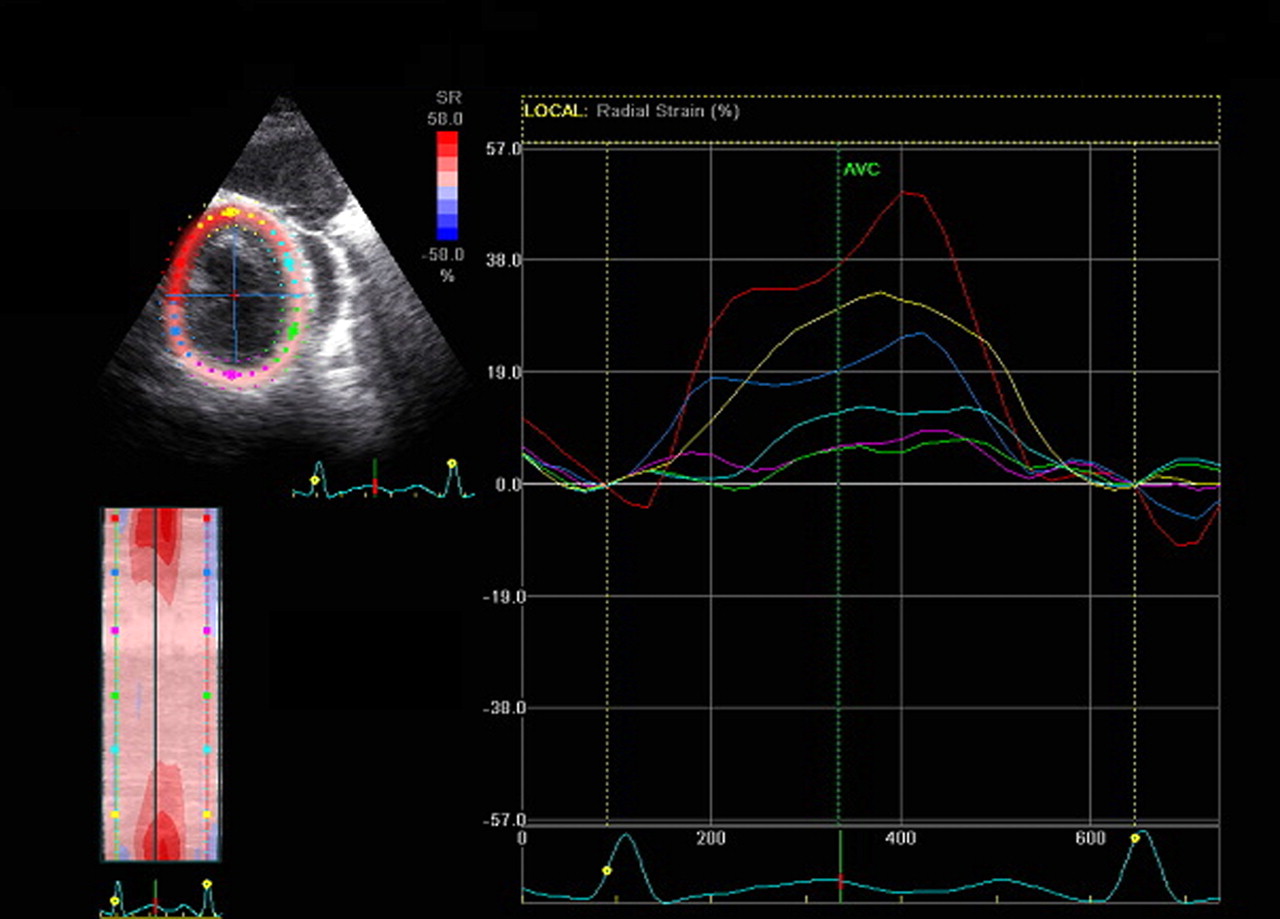
Reduced systolic radial strain rate of anterior and lateral left ventricular walls (light blue and green lines).
The type of cardiac involvement described herein is extremely unusual, including (a) direct compression of the RVOT with superior vena cava syndrome and presyncopes; (b) indirect compression of LA as the extracardiac mass pushes the aortic root against it, causing extreme fatigue; (c) pericardial effusion and (d) reduced systolic strain of left ventricular wall segments contiguous with the extracardiac mass translating possible infiltration or limitation of contraction by external pressure. Echocardiographic strain imaging may help quantify regional myocardial dysfunction in the case of cardiac compression by a mediastinal tumour.
Learning points
Mediastinal masses may present as syncopal or presyncopal episodes due to compression of heart chambers.
Superior vena cava syndrome is a possible manifestation of a non-Hodgkin's lymphoma presenting as a mediastinal mass.
Echocardiographic strain imaging has an emerging role for the detection of subclinical cardiac involvement in many disease processes, including lymphomas or other tumours with cardiac involvement.
This case emphasises the importance of multimodality imaging for a better understanding of the anatomy, degree and extent of cardiac involvement by mediastinal masses.
Footnotes
Competing interests None.
Patient consent Obtained.