Article Text

Statistics from Altmetric.com
Description
‘Typhlitis’ describes enterocolitis of the ileocaecal region seen commonly in neutropenic patients. As compared with other malignant conditions, acute myeloid leukaemia (AML) is most often associated with typhlitis.1 The pathogenesis of typhlitis probably involves a combination of factors, including mucosal injury by cytotoxic drugs, profound neutropenia and impaired host defence to invasion by microorganisms.2 The most common chemotherapeutics associated with typhlitis are cytarabine and daunorubicin.1 Peritonitis and perforation are common complications of typhlitis and surgical intervention is indicated for these patients.3
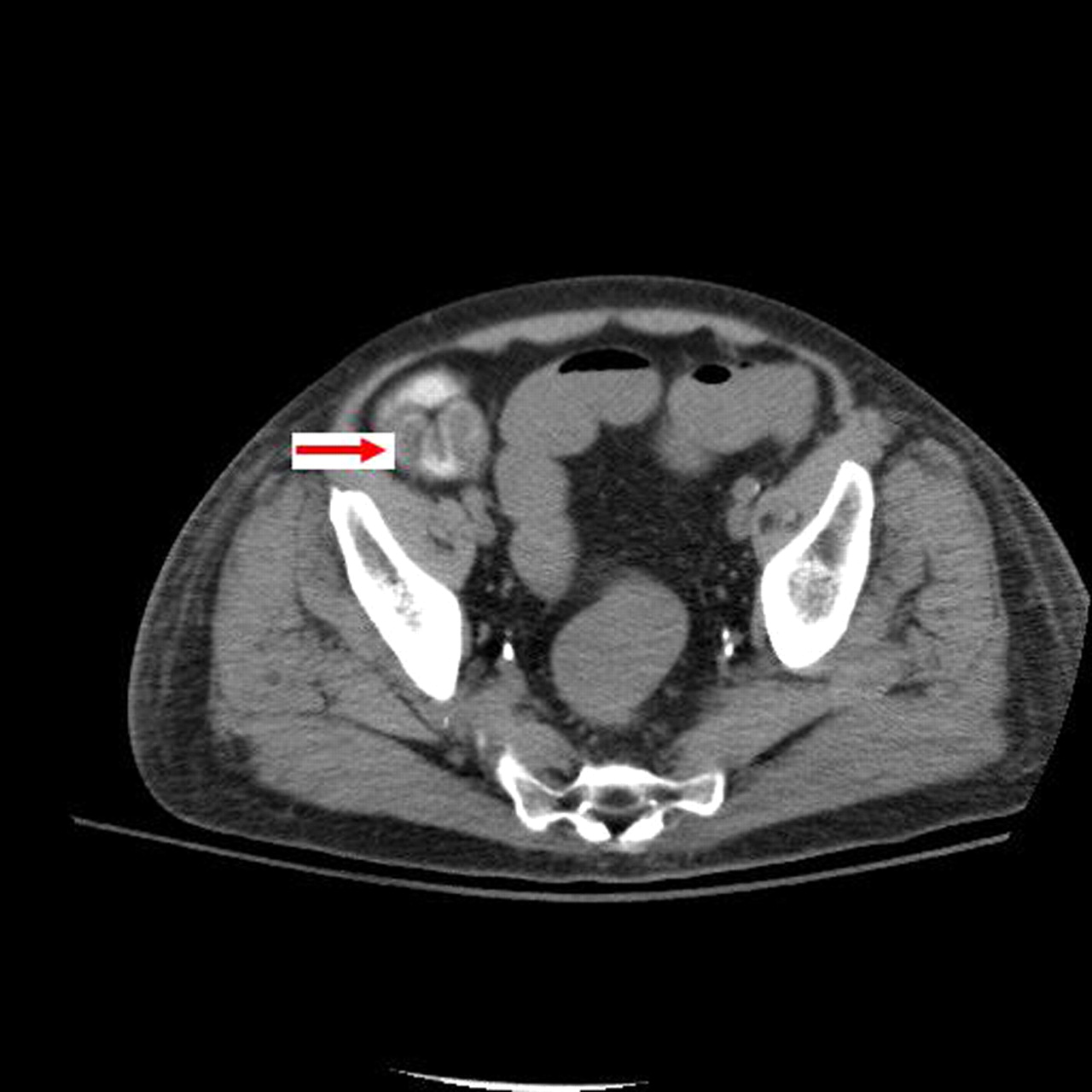
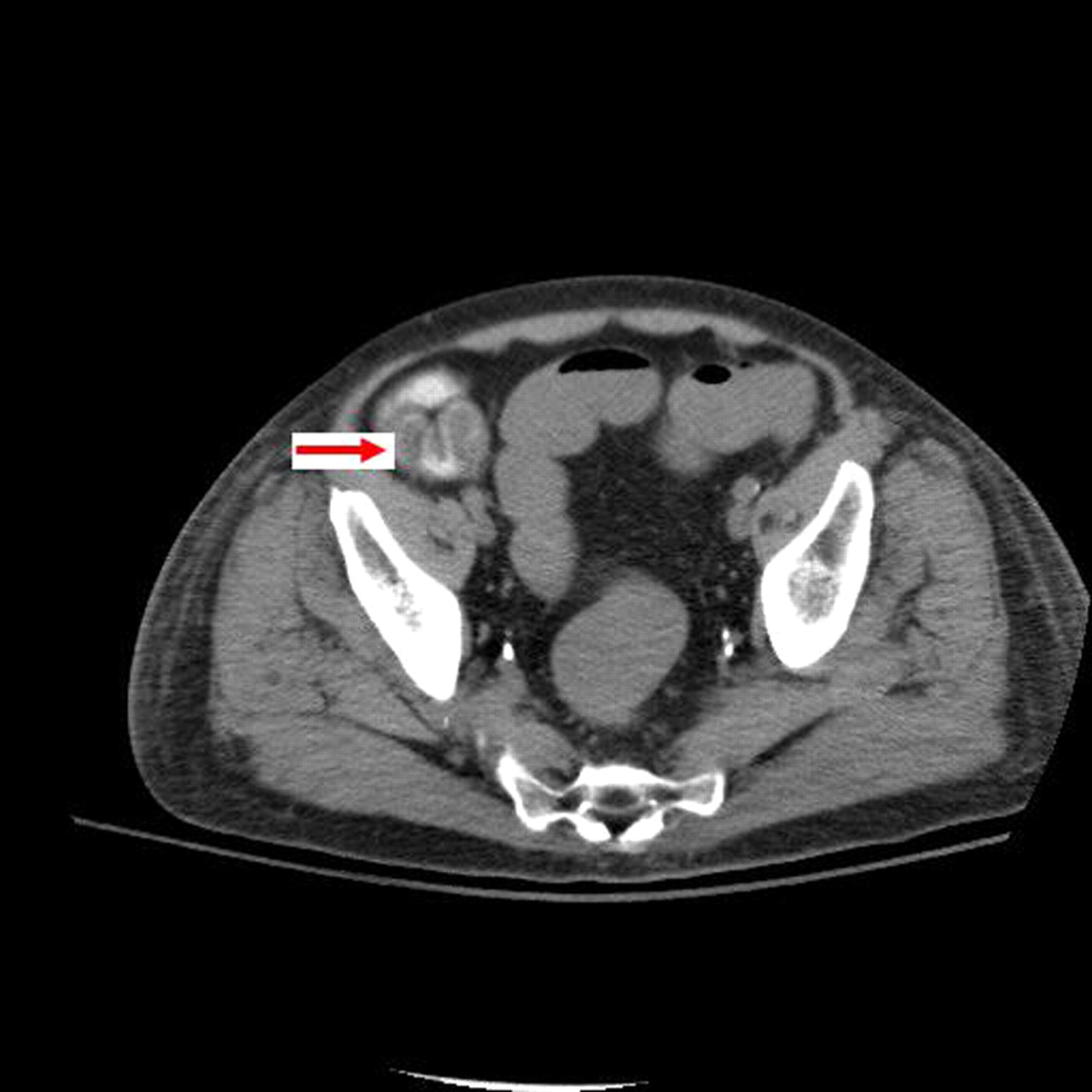
The author reports a 59-year-old man diagnosed with AML and had completed induction chemotherapy consisting of cytarabine and daunorubicin. The patient presented to the hospital with fever and right lower quadrant abdominal pain. Laboratory investigations showed the presence of granulocytopenia with white cell count of 220 cells/mm3 and the absence of neutrophils. The CT scan of the abdomen performed to investigate the abdominal pain demonstrated inflammatory stranding in the mesenteric fat surrounding the small bowel along with a small amount of fluid around the loops of the small bowel (figure 1). Luminal narrowing and mucosal irregularity were evident in the terminal ileum and the caecum (figure 2). These radiological findings have been shown to be highly suggestive of typhlitis.4 Pseudomembranous colitis was differentiated from typhlitis because of localized small bowel involvement, as seen in the later along with negative stool study.4 The patient was treated non-surgically with bowel rest, intravenous fluids, nutritional support and a broad spectrum of antibiotics including antifungal agents. The granulocyte colony-stimulating factor was used to speed up leucocyte recovery and the patient's abdominal condition recovered with improvement in neutrophil count.

CT scan of abdomen showing inflammatory stranding in the mesenteric fat surrounding the small bowel.
{kind=link}
{kind=link}
CT scan of abdomen showing mucosal thickening.
Learning points
Typhlitis’ describes enterocolitis of the ileocaecal region seen commonly in neutropenic patients.
The pathogenesis of typhlitis probably involves a combination of factors, including mucosal injury by cytotoxic drugs, profound neutropenia and impaired host defence to invasion by microorganisms.
Imaging studies suggestive of Typhlitis include diffuse cecal wall thickening; presence of intramural edema and inflammatory stranding in the mesenteric fat surrounding the small bowel.
Footnotes
Competing interests None.
Patient consent Obtained.