Article Text

Statistics from Altmetric.com
Description
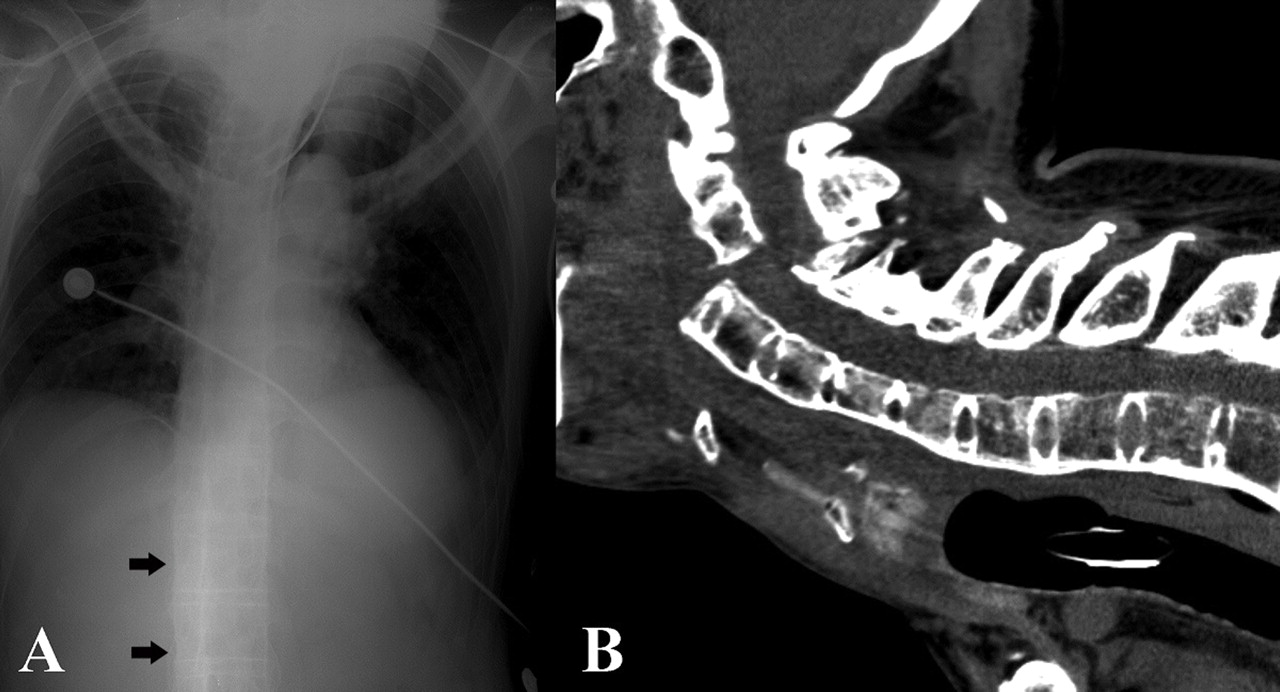
A middle-aged man with an unknown medical history presented to the emergency department with a cardiac arrest. Six hours before symptom onset, the patient had fallen down the subway steps. After the fall, he picked himself up and returned home without any help. The patient went to sleep; 3 h later he was found unconscious by a family member. On admission, the ECG was flat. Five minutes after cardiopulmonary resuscitation, the patient maintained a sinus rhythm. On neurological examination, the patient was in a coma and did not show any response to painful external stimuli. A chest radiograph (figure 1A) and brain CT scan were unremarkable. Severe fluctuations in the blood pressure, pulse rate and body temperature were observed during the intensive care treatment. Follow-up neurological examination 2 days after symptom onset, showed an alert patient that could understand and respond appropriately to verbal commands. The patient could communicate without any difficulty by moving his eyes in all directions. An emergency CT of the cervical spine showed a fracture with severe displacement at the lower C2 level. Diffuse ankylosis of the spine suggested ankylosing spondylitis (AS) (figure 1B). Careful review of the initial chest radiograph suggested a bamboo spine (figure 1A). The patient remained in a locked-in state during the next 4 days and died after another a cardiac arrest. AS is a chronic, progressive inflammatory disease that primarily affects the axial skeleton.1 It is characterised by ossification of the spinal discs, joints and ligaments that lead to progressive rigidity and altered biomechanical properties of the spine. Patients with AS are at a higher risk of spinal fracture and up to 75% of fractures develop in the cervical spine. Falls are the most common cause of fracture and associated neurologic deficits can be subtle.2 Locked-in syndrome is frequently mistaken for a coma. The patient is awake but speechless and motionless, with little response to stimuli. A brainstem stroke is the major cause of the locked-in syndrome; however, it may occur after any significant trauma. Even for experienced clinicians, it can be difficult to diagnose cognitive ability in the presence of profound physical disabilities. Inadequate awareness and inappropriate management of the injuries may have significant consequences. A thorough history and careful physical examination are required in patients with AS.3

{kind=link}
A chest radiograph and emergency CT of the cervical spine. (A) Careful review of the initial chest radiograph suggesting a bamboo spine (arrows). (B) Emergency CT of the cervical spine showing a fracture with severe displacement at the lower C2 level, anterior to the body of the spinous process involving a facet joint fracture and diffuse ankylosis of the cervicothoracic spine.
Footnotes
-
Competing interests None.
-
Patient consent Not obtained.