Article Text

Statistics from Altmetric.com
Description
Following a seemingly straightforward procedure to place the necessary applicators (comprising the central tandem into the uterine cavity, and the right and the left ovoids into the lateral vaginal fornices), this patient of cervical-carcinoma, who was scheduled to receive intracavitary brachytherapy (ICBT) was taken up for CT scanning intended for dose-optimised three-dimensional conformal brachytherapy.
Surprisingly, it was noted that the central tandem had pierced through the posterior wall of the uterus to enter the abdominal cavity (figures 1⇓–3). The uterine body was visualised as anteflexed, even though a preprocedure clinical examination was not suggestive of the same. The applicators were removed, and the procedure was postponed.

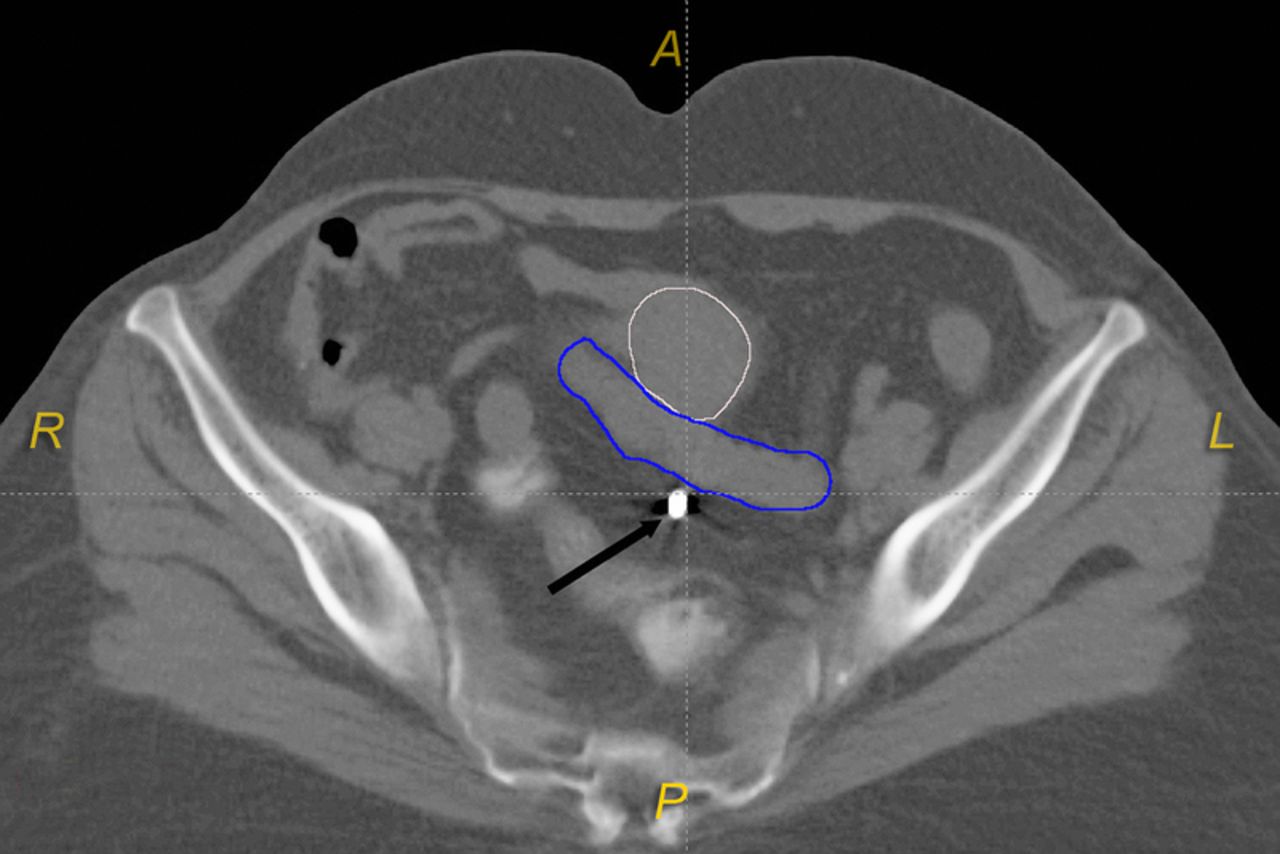
Axial CT slice demonstrating the location of the uterine tandem (black arrow), the uterus (outlined in white) and a loop of small intestine (outlined in blue) which could have been exposed to radiation overdose if not for the discovery of the applicator malposition.
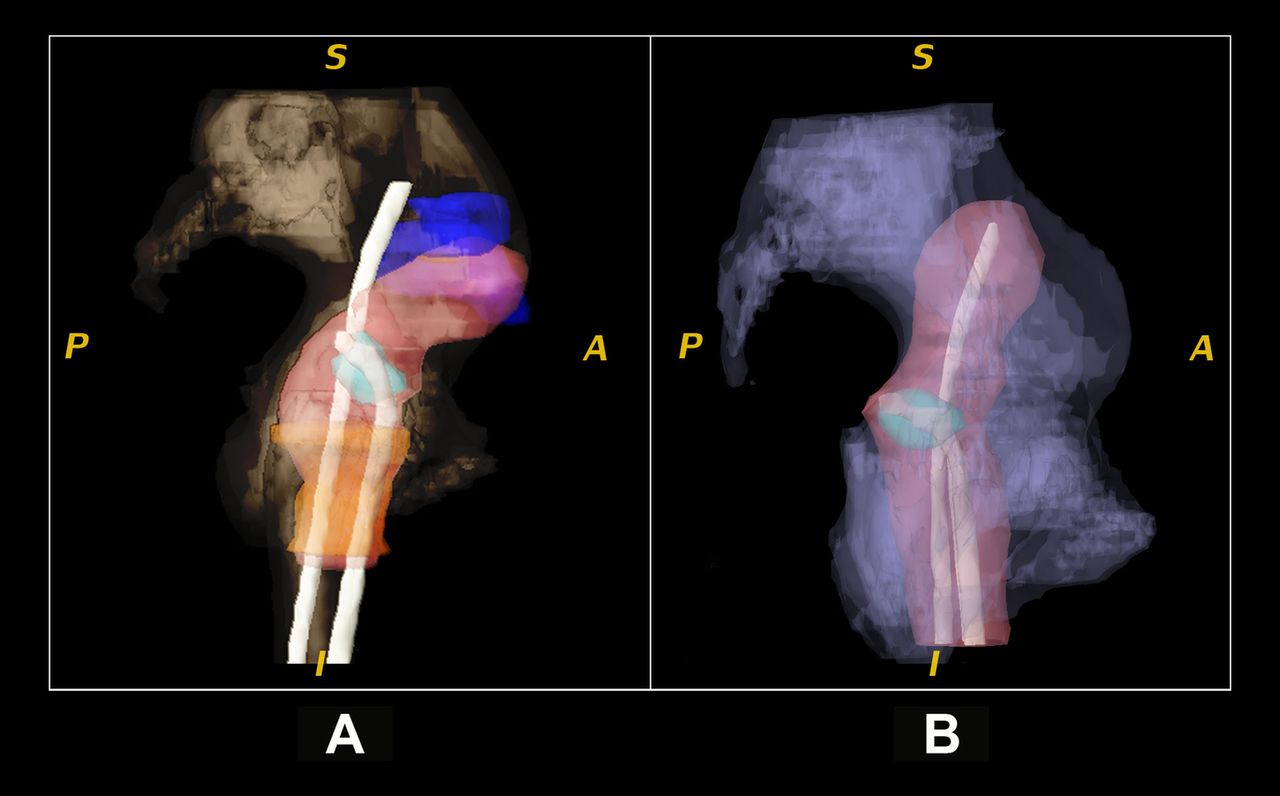
(A) Digital volumetric reconstruction of the CT scan depicting the relative positions of the uterine tandem with the small bowel (blue) the uterine body (pink); (B) A correct application shown for depicting the intended position of the uterine tandem, within the uterus.

{kind=link}
{kind=link}
{kind=link}
(A) Digital volumetric CT reconstruction showing the relative positions of the applicators and the pelvic structures. (B) A two-dimensional x-ray radiograph would not have indicated the malposition of the uterine tandem.
Successful radiotherapy for cervical carcinoma typically requires the integration of brachytherapy with external-beam radiotherapy. Brachytherapy allows adequate dosing of the uterus, upper-vagina, cervix and a small area of adjoining parametrium, while at the same time sparing the urinary bladder and rectum from excessive doses. ICBT is a time-tested treatment for cervical carcinoma, wherein the accessible utero-cervical cavity is irradiated from-within by the placement of applicators to facilitate radioactive-source loading.
With regard to applicator placement, even though ultrasound-guidance is known to reduce the risk of uterine perforations, it remains unadopted by a majority of clinicians. This report illustrates the potential benefit that could have been had with ultrasound-guidance.1
In the current era, the applicators are loaded with a computer-controlled iridium-192 source which delivers the radiation. After the placement of the tandem and ovoids, the dose-optimisation is usually done either with a traditional ‘x-ray simulation’ or with a ‘CT-simulation’. Though the x-ray simulation is simple and less-expensive, CT-simulation is clinically advantageous as it provides an opportunity for volumetric dose-optimisation. The current case demonstrates another advantage, that is, the possible detection of unexpected uterine perforations.2 ,3
Learning points
-
Given that the tissues could be friable and prone to perforations owing to the cancer itself and the usual use of prior external beam radiotherapy, the potential risk of uterine perforation should not be underestimated.
-
The use of ultrasound-guidance during applicator placement may reduce the risk of uterine perforations.1
-
The use of traditional x-ray simulations may make the planner oblivious to the true position of the central tandem, which if loaded in the intra-abdominal location could expose the small intestine to risk of serious radiation dosages.3
-
The use of CT scan after application not only allows for volumetric dose-optimisation, but also allows the detection of applicator mal-placements, as illustrated by this report.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.