Article Text

Statistics from Altmetric.com
Description
As part of a routine assessment for liver transplantation, a 48-year-old gentleman with cirrhosis secondary to hepatitis C (genotype 2b) underwent intra-abdominal imaging. His indications for liver transplantation were recurrent ascites with diuretic intolerance and episodes of spontaneous bacterial peritonitis as well as a high UK model for end-stage liver disease score (UKELD of 57). He had also had two previous episodes of variceal bleeding necessitating band ligation and stays in intensive care.
A triple phase liver CT showed liver cirrhosis and ascites. It also identified a hypodense appearance of the main portal vein extending into the right and left main branches, believed to represent a large filling defect (figure 1). Consequently, the diagnosis of portal vein thrombosis was made. This condition has an increased incidence in patients with liver cirrhosis and is a relative contraindication to liver transplantation.

Axial plane triple phase CT liver examination demonstrates a hypodense main portal vein (arrows) proximal to the confluence of the splenic and superior mesenteric veins (A) arterial phase (B) portovenous phase (C) delayed phase (D) coronal plane portovenous phase (note large volume ascites).
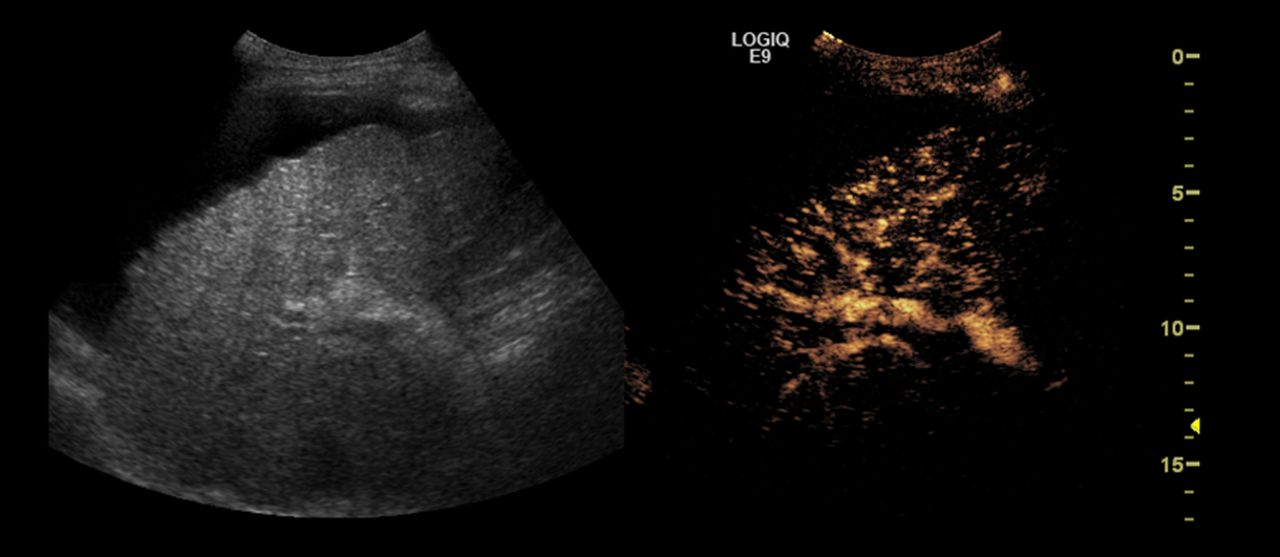
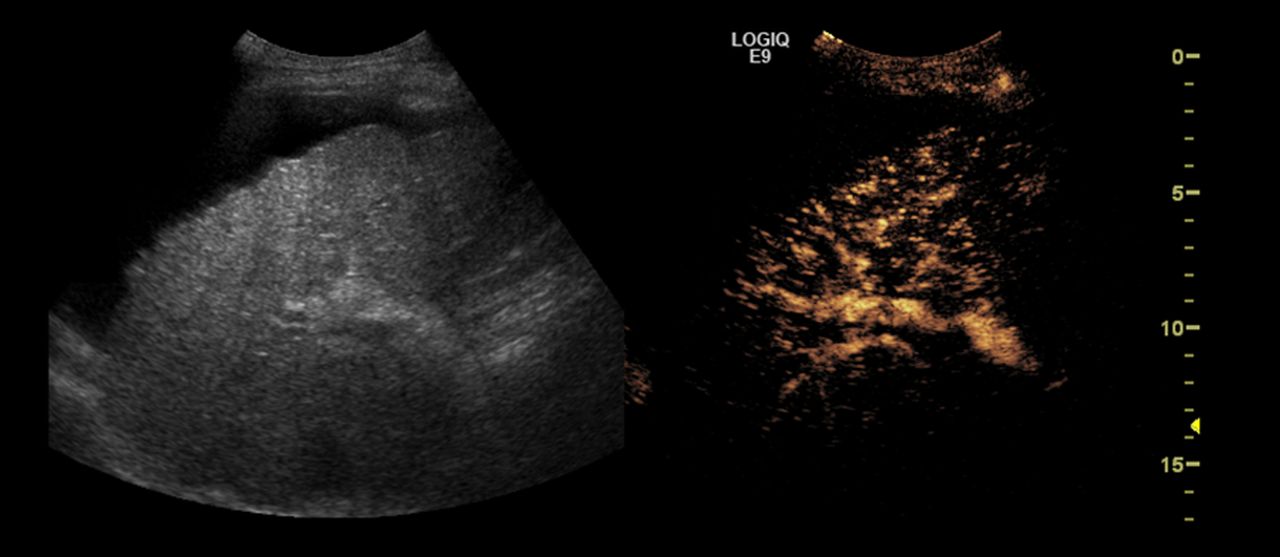
Soon after this, the patient was referred for ultrasound-guided drainage of his tense ascites. As part of the initial assessment, the portal vein was noted to be patent. No thrombus was identified. To further investigate this unexpected finding, a contrast ultrasound study using intravenous sulphur hexafluoride microbubbles, confirmed good portal vein opacification and no thrombus (figure 2). The patient had not been anticoagulated between the CT and ultrasound scan which were 4 weeks apart. The patient remained on the liver transplant waiting list.
{kind=link}
{kind=link}
Left: the grey-scale ultrasound shows a coarsened liver echotexture with a nodular outline and ascites in keeping with cirrhosis. Right: contrast microbubble enhanced liver ultrasound shows portal vein opacification. No portal vein thrombus identified.
Learning points
-
Opacification of the portal vein on CT relies on normal hepatopetal flow of contrast from splanchnic circulation and normal portal venous blood pressure.1 ,2
-
In patients with liver cirrhosis and portal venous hypertension, large filling defects in the portal vein on CT could represent flow artifacts or thrombus. Differentiation between these entities using US Doppler or contrast-enhanced US is important as it alters the management.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.