Article Text

Statistics from Altmetric.com
Description
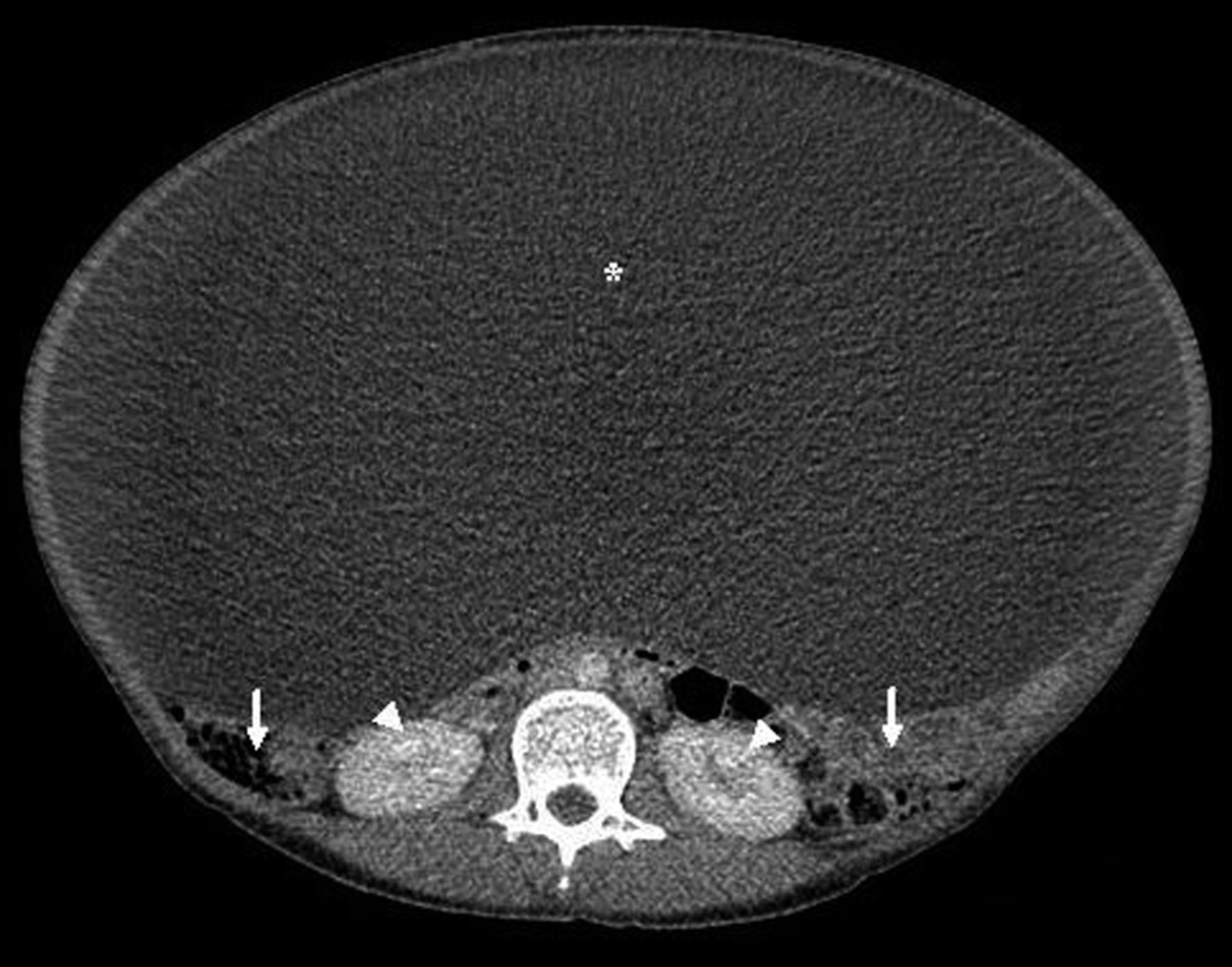
A 36-year-old woman with no medical history (gravida 0, para 0) was admitted in the hospital because of progressive abdominal distension for several months. Physical examination revealed an enlargement of the abdomen, without other abnormalities. Laboratory findings were unremarkable. The diagnosis of ascites was proposed initially. A trans-parietal punction revealed a clear fluid, with no cells and a protein concentration of 1 g/l. The fluid was sent for culture and bacteriological testing and turned out to be sterile. Abdominal CT (figure 1) finally disclosed a large well-limited and encapsulated mass of 41×42×24 cm (asterisk), which seemed to originate from one of the ovaries, repressing the bowel (arrow) and the kidneys (arrow head), without signs of bowel obstruction or hydronephrosis. Tumour markers (CA19·9, CA125, α-fetoprotein and carcinoembryonic antigen) were normal. A laparotomy disclosed a voluminous left ovarian cyst, which was punctured (23 l) and extracted during a left adnexectomy. Postoperative course was uneventful and the patient was discharged home. Pathological examination revealed a benign serous ovarian cystadenoma, with no evidence for malignancy.
{kind=link}
Abdominal CT showing a large ovarian cyst (41×42×24 cm, asterisk) repressing the bowel (arrows) and the kidneys (arrow heads).
Mainly described in the literature as case reports,1 giant ovarian cysts are often misdiagnosed as ascites following the initial clinical and even sonographic evaluation. The growth rate of ovarian cystadenoma, the most common benign ovarian neoplasm, is usually described as very slow.2 Similar conditions may arise from omentum, mesenterium and retroperitoneal structures. Giant ovarian cysts are usually managed by laparotomy and ovariectomy, although laparoscopic ovariectomy has been proposed.3
Learning points
-
Giant ovarian cysts are frequently misdiagnosed as ascites and should always be considered in differential diagnosis of abdominal cavity enlargement.
-
Initial sonographic evaluation can fail to diagnose correctly a giant ovarian cyst.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.