Article Text

Statistics from Altmetric.com
Description
These are images of an elderly man presenting with back pain, weight loss and diarrhoea. Clinical examination revealed peripheral oedema, pan-systolic murmur and a non-tender mass in his left iliac fossa. Abdominal CT revealed a calcified mass in the left iliac fossa with a characteristic spoke wheel appearance of carcinoid tumour (see arrow in figure 1) and solid and cystic liver lesions, consistent with multiple metastases.

Abdominal CT scan.
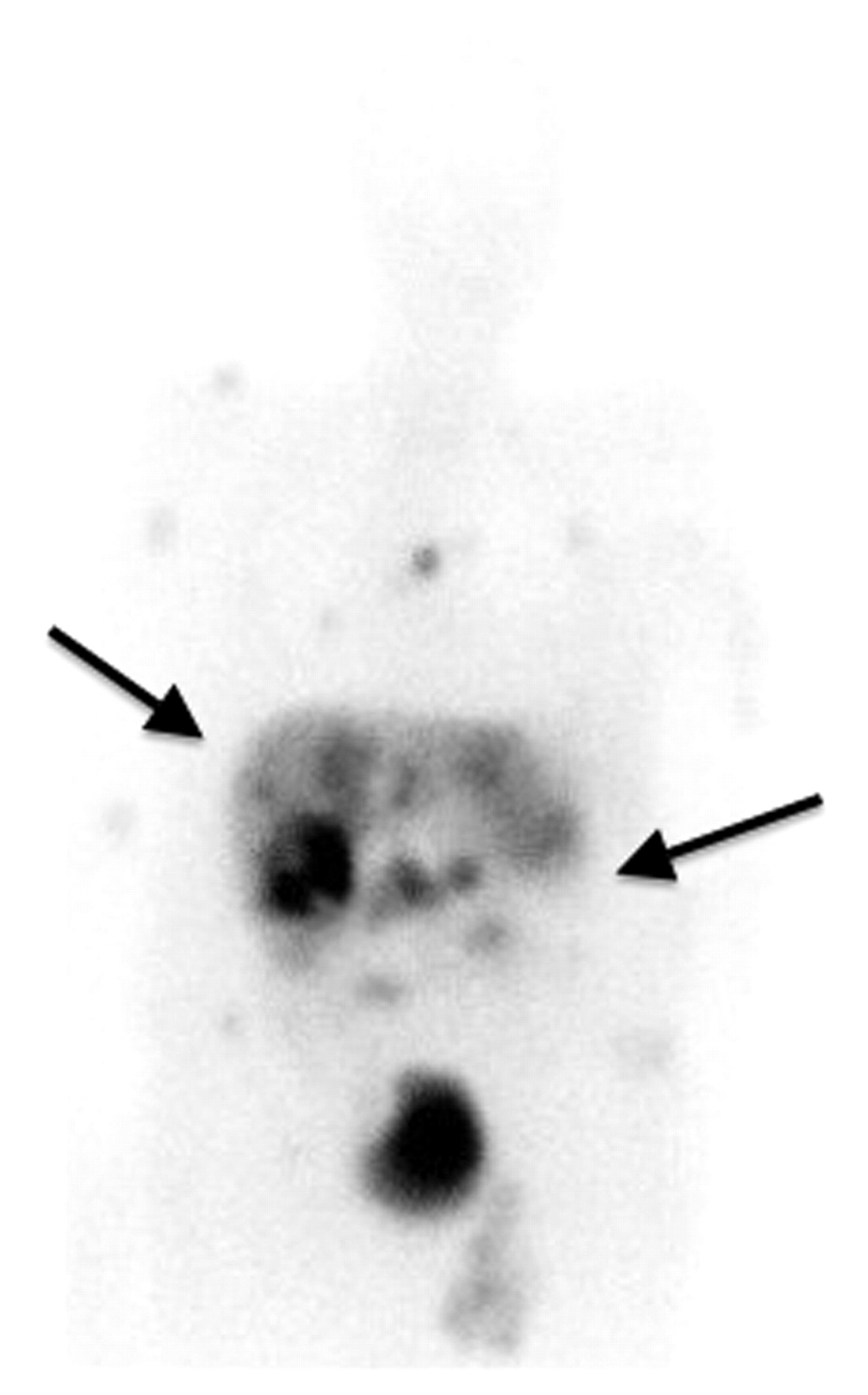
An 111In-Octreotide examination demonstrated somatostatin-receptor-positive metastatic disease in the liver, abdominal lymph nodes and abnormal uptake in the bones, suggesting widespread skeletal metastases (figure 2 shows tumour sites identified by uptake of Octreotide, arrows indicate hepatic metastases and small bowel tumour). Transthoracic echocardiography revealed a thickened, immobile tricuspid valve, with mild tricuspid stenosis and severe regurgitation (figure 3; dense continuous wave Doppler signal through tricuspid valve representing severe tricuspid regurgitation).

111Indium-Octreotide scan.

{kind=link}
{kind=link}
{kind=link}
Transthoracic echocardiogram; continuous wave Doppler through a tricuspid valve.
Unfortunately, despite treatment, the patient died during the same hospital admission.
Neuroendocrine tumours are rare (incidence: 1.2–2.1 per 100 000 of the general population per year1) malignancies originating from the enterochromaffin cells in the gastrointestinal tract, causing the release of vaso-active substances into the systemic circulation. The most common sites are the terminal ileum and appendix and up to 22% have evidence of liver metastases at diagnosis.2
Multiple imaging modalities assist in both the diagnosis of carcinoid disease and its complications. Large tumour burden, widespread disease and carcinoid heart disease are poor prognostic indicators, and as typified by our patient, a poor outcome is almost inevitable with the combination of these factors.
Learning points
An Octreoscan is a functional imaging modality that may be useful in localising the primary tumour site and in determining the extent of tumour burden in patients with neuroendocrine tumours.
The combination of different imaging modalities may provide complementary information regarding disease burden and its multiple complications.
Large tumour burden, widespread disease and carcinoid heart disease are poor prognostic indicators, and a poor outcome is almost inevitable with the combination of these factors.
Footnotes
Competing interest None.
Patient consent Obtained.