Article Text

Statistics from Altmetric.com
Description
Gossypiboma is the term for a surgical swab accidentally left inside a patient's body. It is derived from the Latin word ‘gossypium’ meaning cotton and the Swahili ‘boma’ meaning place of concealment.1 Gossypiboma has an incidence of 1:1500 for intra-abdominal operations.2 Common presentations of gossypiboma are abdominal distension, ileus, tenesmus, pain, palpable mass, vomiting, weight loss, diarrhoea, abscess and fistula formation.3 In addition to the physical and psychological impact on the patient, retained surgical equipment cost the National Health Services the equivalent of $12.8 million over the past 5 years (figures 1 and 2).

The swab protruding into the rectum.
{kind=link}
{kind=link}
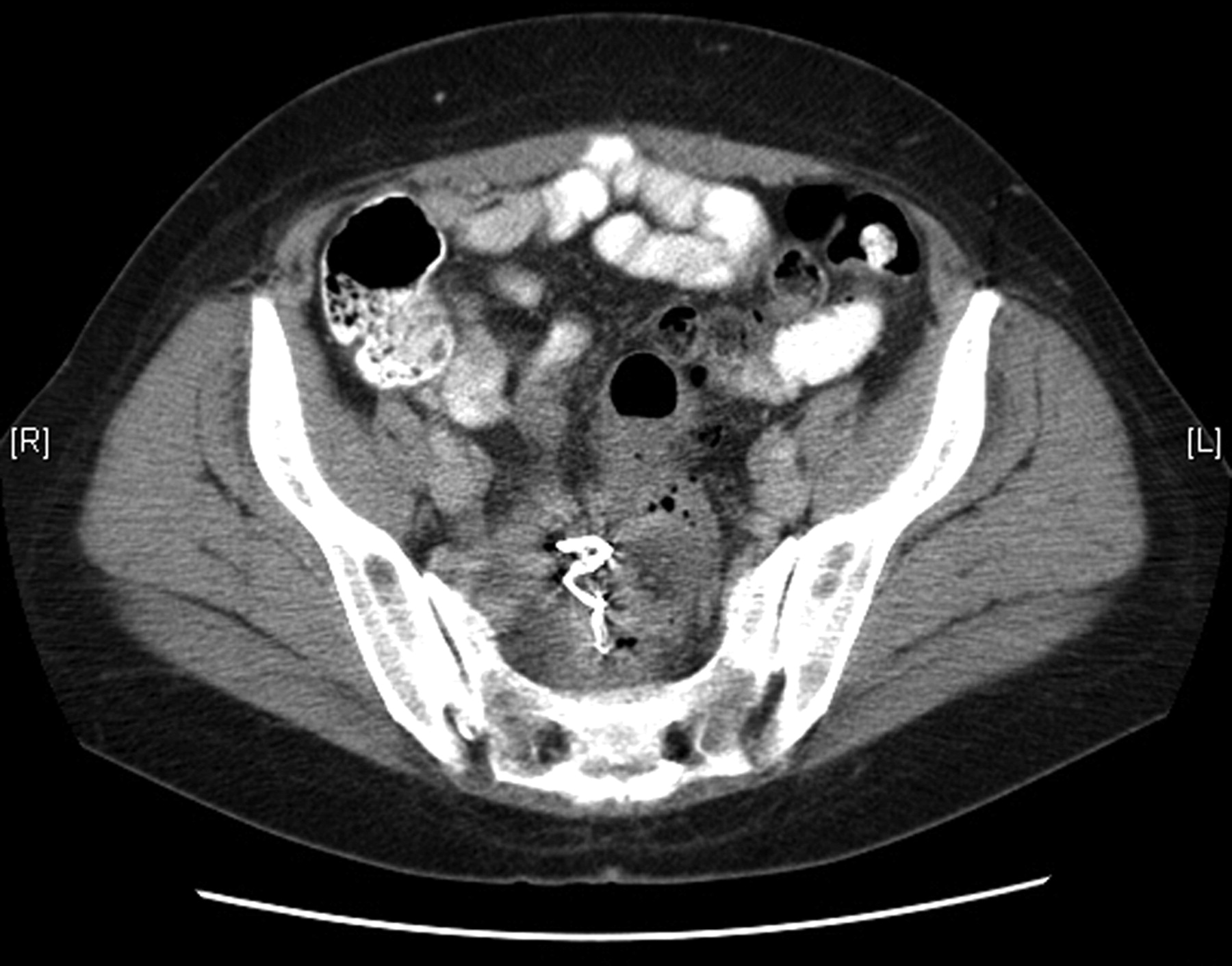
CT image showing the retained foreign body.
A 56-year-old woman presented with alteration of bowel habit 6 months after sacrohysteropexy. The swab was seen on CT in the pelvic cavity surrounded by a collection 15 cm above the anus and boring its way into the rectum. The swab was successfully removed by rigid sigmoidoscopy using a laparoscopic grasping forceps thus avoiding a laparotomy and avoiding a defunctioning colostomy. The patient had the procedure under general anaesthetic and was consented for laparotomy. The patient had an uneventful postoperative period with improvement of her symptoms. We have followed her up for 5 months and there was no development of pelvic sepsis.
To the best of our knowledge there are no other cases in the literature where a missed swab was removed by sigmoidoscopy.
Unfortunately, most reported cases of gossypiboma, despite being a ‘never event’, occur in the presence of a normal pack count which underlines the necessity of vigilance of all theatre staff to prevent this avoidable complication.
Learning points
In order to avoid gossypiboma, one cannot put enough emphasis on thorough swab counting. The golden dictum stating that prevention is better than cure invariably applies to all cases of gossypiboma.
Despite thorough swab counts, the diagnosis of gossypiboma should be borne in mind in patients with a history of previous surgery.
In selected cases where the swab has started to penetrate the wall of the intestine, an attempt of removal through sigmoidoscopy might spare the patient a laparotomy.
Footnotes
Contributors All authors have equally contributed to this submission.
Competing interests None.
Patient consent Obtained.