Article Text

Statistics from Altmetric.com
Description
A 61-year-old man was referred to our rheumatology unit with a 3-month history of worsening left-sided neck and shoulder pain. His general practitioner (GP) suspected Giant cell arteritis and a temporal artery biopsy was performed which was negative. Shoulder and neck x-rays were also normal. He had a 40-pack-year smoking history and a chest radiograph was organised by his GP. On questioning, he admitted to significant weight loss and hoarseness of voice.
On examination, shoulder movements did not exacerbate his pain and he had a full range of shoulder and upper-limb movements. He had a left Horner's syndrome, a cyanosed left forearm with feebly palpable left upper-limb pulses. The temporal arteries were non-tender. Chest examination was unremarkable. His erythrocyte sedimentation rate and C-reactive protein level were raised at 30 mm/h and 60 mg/l, respectively. Other blood tests were unremarkable.
A chest radiograph (figure 1) showed slight right-sided tracheal deviation and subtle non-homogenous left upper-lobe opacity. The history and clinical features along with radiological findings were highly suggestive of a left apical lung lesion. An urgent enhanced CT scan of the thorax (figures 2 and 3) was arranged and demonstrated a soft-tissue mass (6.9 cm × 5.4 cm × 7.7 cm) in the left lung apex encasing the left subclavian artery.

Chest radiograph with slight right tracheal deviation and subtle non-homogenous opacity in left upper zone (black arrows).
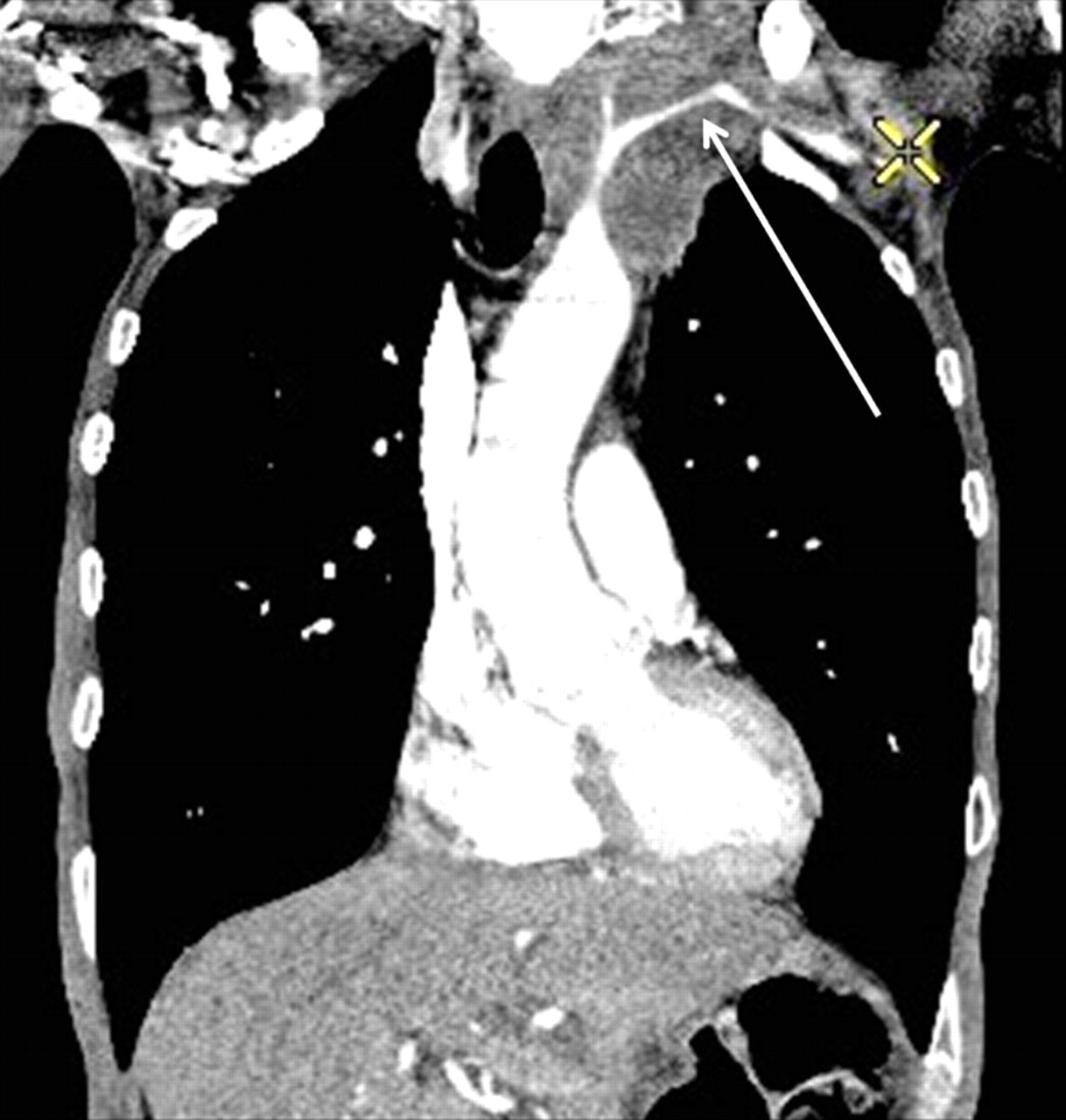
Coronal enhanced CT scan image of the thorax demonstrates a soft-tissue mass (6.9 cm × 5.4 cm × 7.7 cm), in left lung apex encasing the subclavian artery (white arrows).

{kind=link}
{kind=link}
{kind=link}
Sagittal enhanced CT scan image of the thorax shows encased subclavian artery by a Pancoast tumour (white arrows).
Of the patients presenting with a Pancoast tumour, 1.7% have a normal plain chest radiograph.1 Our case illustrates that when there is a high index of clinical suspicion, CT imaging should be undertaken to exclude a Pancoast tumour even when the plain radiograph changes are subtle.
Shoulder pain has been reported as being the first presenting feature of a Pancoast tumour in 90% of cases.2 It is of interest that the original description of a Pancoast tumour in 1932 by Henry Pancoast3 was of shoulder pain due to an apical mass.
Footnotes
Competing interests None.
Patient consent Obtained.