Article Text

Statistics from Altmetric.com
Description
A 76-year-old man presented to our hospital with complaints of left-sided distention of the abdomen and gross haematuria. The patient's medical history included coronary artery disease, hypertension, predialytic chronic kidney disease and abdominal aortic aneurism (AAA). One month prior to current admission the patient was started on haemodialysis. At physical examination there was a prominent swelling on the left side of the abdomen. The mass was not pulsatile. Coronal maximum intensity projection (MIP) image showed (figure 1) partially thrombosed saccular aneurism which fills left side of the abdominal cavity (red arrows), and partially thrombosed fusiform aneurism in distal aorta (green arrows). Widespread atherosclerotic calcifications are evident on the walls of the abdominal aorta and the iliac arteries. The left kidney was severely displaced by the ruptured AAA. The maximum diameter of the fusiform and saccular parts was 6.4 and 23 cm, respectively. Axial slice of the abdominal CT showed (figure 2) indentation of the ruptured abdominal aneurism to anterior abdominal wall, severe displacement of the kidney towards anterior and inferior by bulky haematoma (red arrows) and a calcul in the pelvis of the left kidney (green arrow). The case was deemed inoperable. The patient underwent heparin-free haemodialysis and repeatedly transfused with RBC suspensions. The patient died at 39th day of hospitalisation.

In coronal MIP image shows partially thrombosed saccular aneurism which fills left side of the abdominal cavity (red arrows), and partially thrombosed fusiform aneurism in distal aorta (green arrows).
{kind=link}
{kind=link}
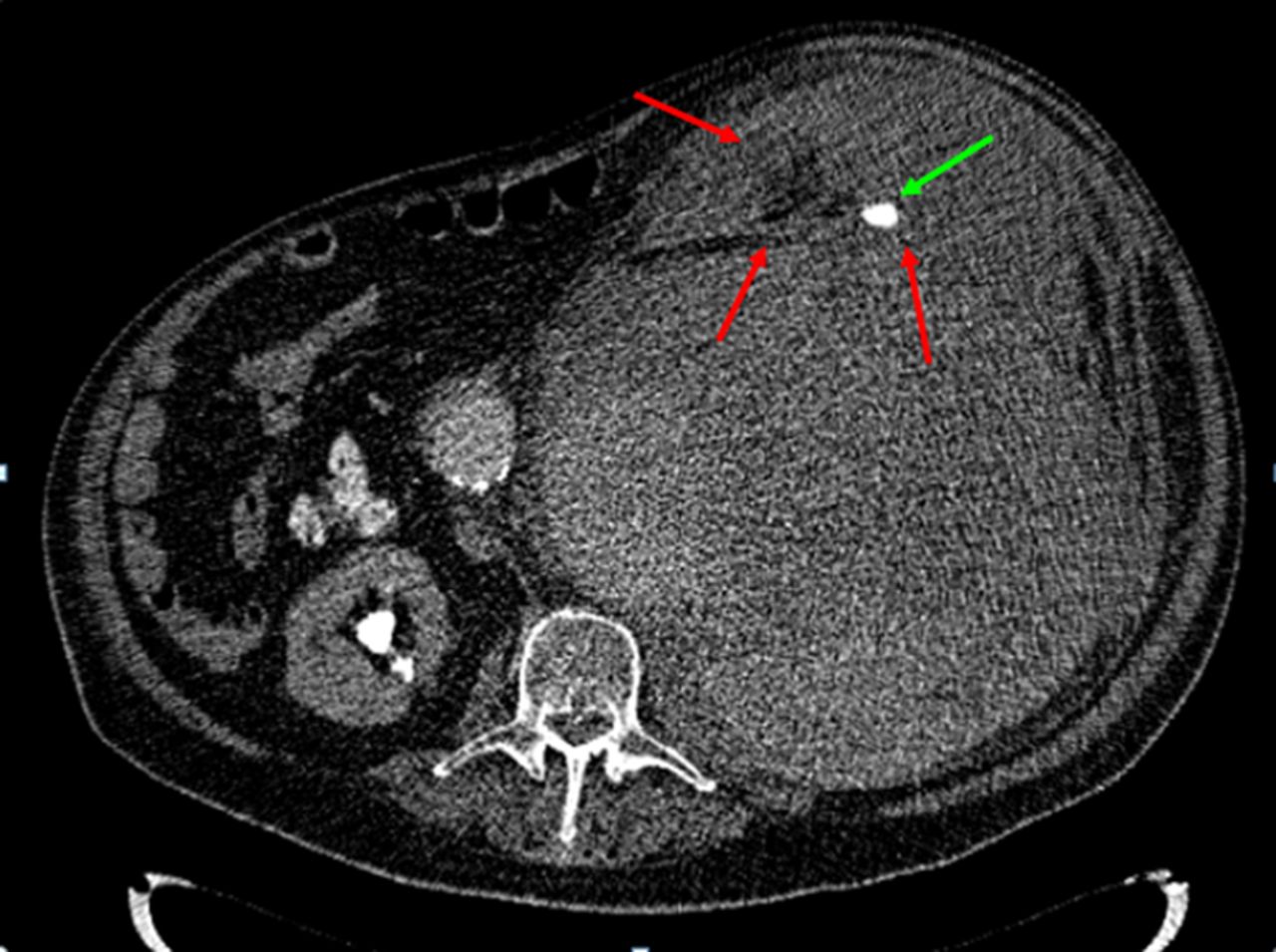
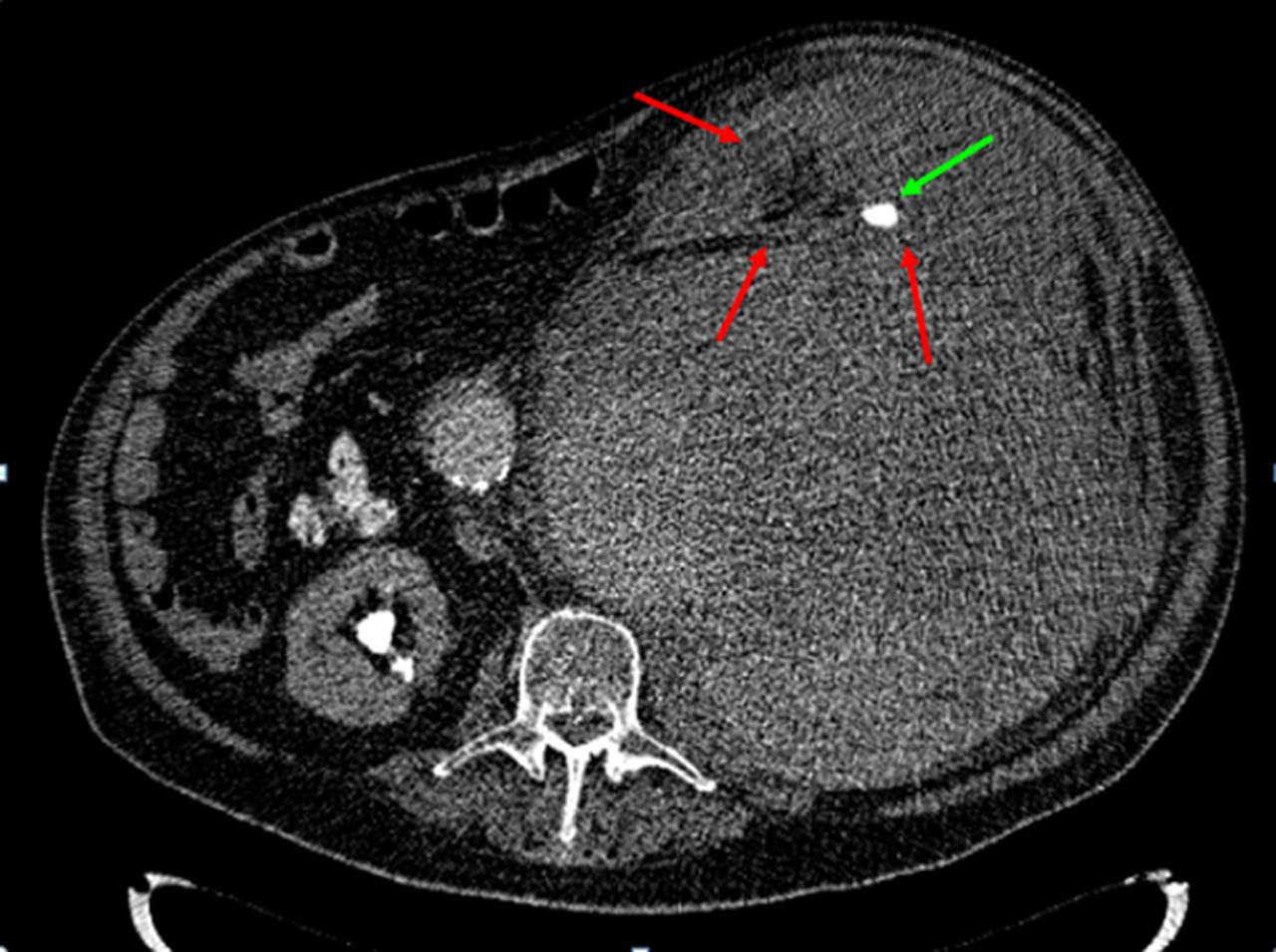
Axial slice of the abdominal CT shows indentation of the ruptured abdominal aneurism to anterior abdominal wall, severe displacement of the kidney toward anterior and inferior by bulky hematoma (red arrows) and a calcul in the pelvis of the left kidney (green arrow).
Ninety-five percent of aortic aneurisms are fusiform in shape and the aetiology is degeneration of the vascular wall. In contrast, saccular aortic aneurisms are much less common and most of the time develop secondary to infection of the aorta.1 Rest of the saccular AAA results from a penetrating aortic ulcer. To the best of our knowledge, coexistence of saccular and fusiform aneurisms contiguously in the same patient has never been reported before. This case illustrates a marginal example of a ruptured AAA. The left kidney was displaced severely towards the anterior abdominal wall by bulky haematoma of the saccular aneurism. While amenable to surgery at first, severely expanded aneurism was deemed inoperable at current admission and the patient succumbed to death due to severe internal bleeding.
Learning points
-
Abdominal aortic aneurism is the life-threatening condition and should be diagnosed as early as possible.
-
Abdominal aortic aneurisms should be repaired surgically before the point of no return.
-
This is the first report of simultaneous presentation of a saccular and fusiform aneurism in the same patient.
Reference
Footnotes
Competing interests None.
Patient consent Obtained.