Article Text

Statistics from Altmetric.com
Description
A 58-year-old woman with autosomal-dominant polycystic kidney disease (ADPKD) and chronic kidney disease presented to our hospital with low-grade fever and severe abdominal distension. Laboratory tests showed a white blood count of 7.9×109/l and haemoglobin level of 7.1 g/dl. The urea nitrogen level was 103 mg/dl; serum creatinine, 2.9 mg/dl; C-reactive protein, 16.1 mg/dl; and soluble interleukin 2 receptor, 6440 U/ml. Abdominal MRI showed massive ascites without any detectable mass or lymphadenopathy (figure 1A,B).

Massive ascites and enlarged polycystic kidney and liver on coronal (A) and axial (B) T2-weighted MRI of the abdomen.
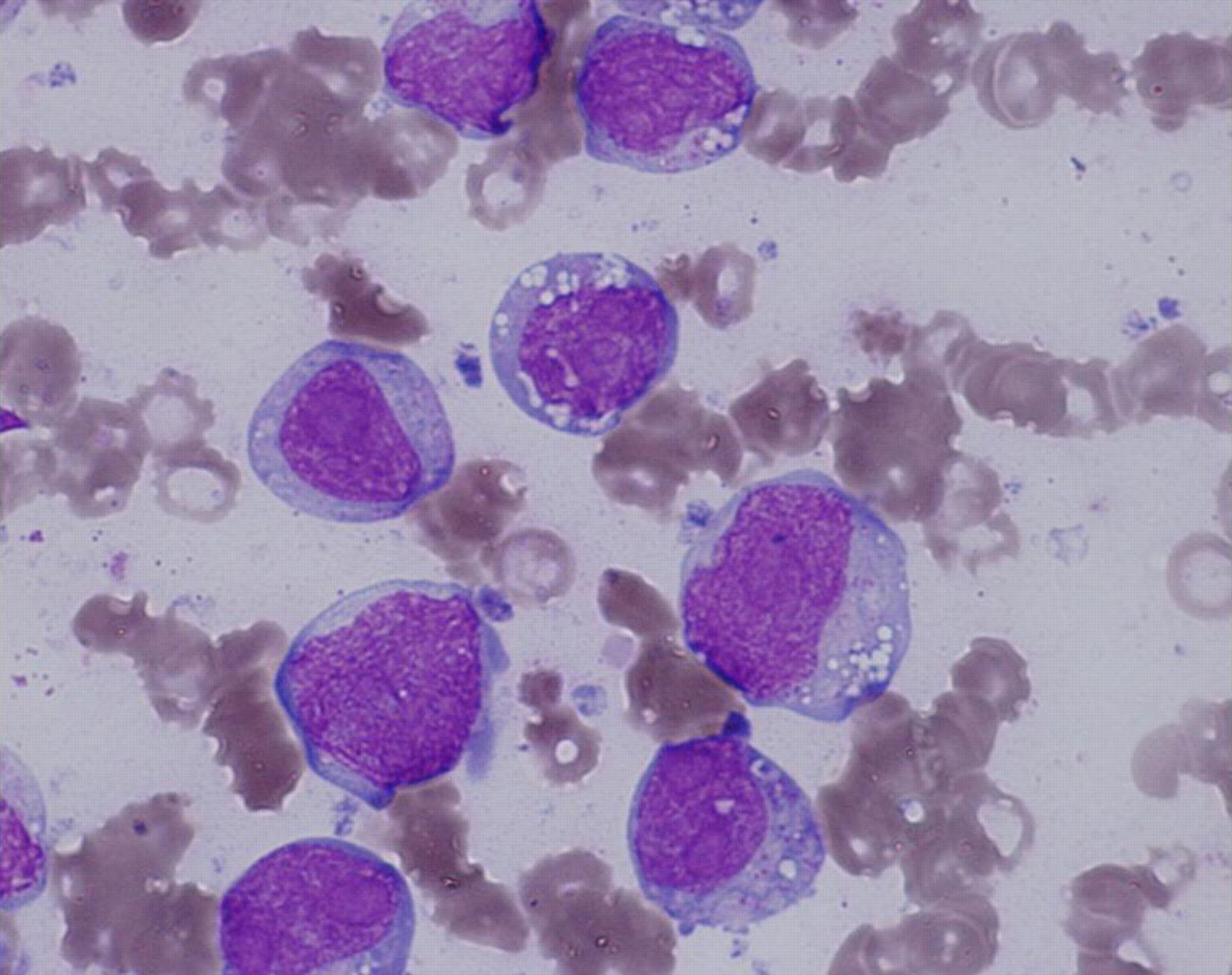
Since the ascites, which were likely because of portal hypertension and latent cyst infection, proved refractory to several diuretics and antibiotics, abdominocentesis was performed. Cytology showed lymphoma cells with large nuclei and abundant cytoplasm with occasional vacuoles, which exhibited a B-cell phenotype (figure 2, Giemsa stain ×1000). She was negative for human herpes virus (HHV)-8 and HIV, and was diagnosed as having HHV-8-unrelated HIV-negative primary effusion lymphoma (PEL)-like lymphoma. The patient was responsive to chemotherapy showing a significant decrease of the massive ascites. However, refractory multiorgan failure developed, and the patient died 1.5 years after diagnosis.
{kind=link}
{kind=link}
Abdominocentesis cytology.
PEL is a rare type of large B-cell lymphoma that is generally confined to the body cavities of immunosuppressed patients infected with HHV-8.1 HHV-8-unrelated PEL, which is referred to as PEL-like lymphoma,2 ,3 in an ADPKD patient is extremely rare and has not been reported yet. It may be important to consider the possible complications of lymphoma and to examine ascites, when refractory ascites is observed in ADPKD patients.
Footnotes
Competing interests None.
Patient consent Obtained.