Article Text

Statistics from Altmetric.com
Description
A 14-year-old boy presented to our emergency department with status epilepticus of 1-h duration. He also had multiple episodes of generalised tonic-clonic seizures and intermittent headache for the past 1 month. He was a school dropout and belonged to a poor socioeconomic background. On examination, he was deeply comatose. Initial investigations included an axial contrast-enhanced CT of the brain subsequently followed by MRI of the brain.
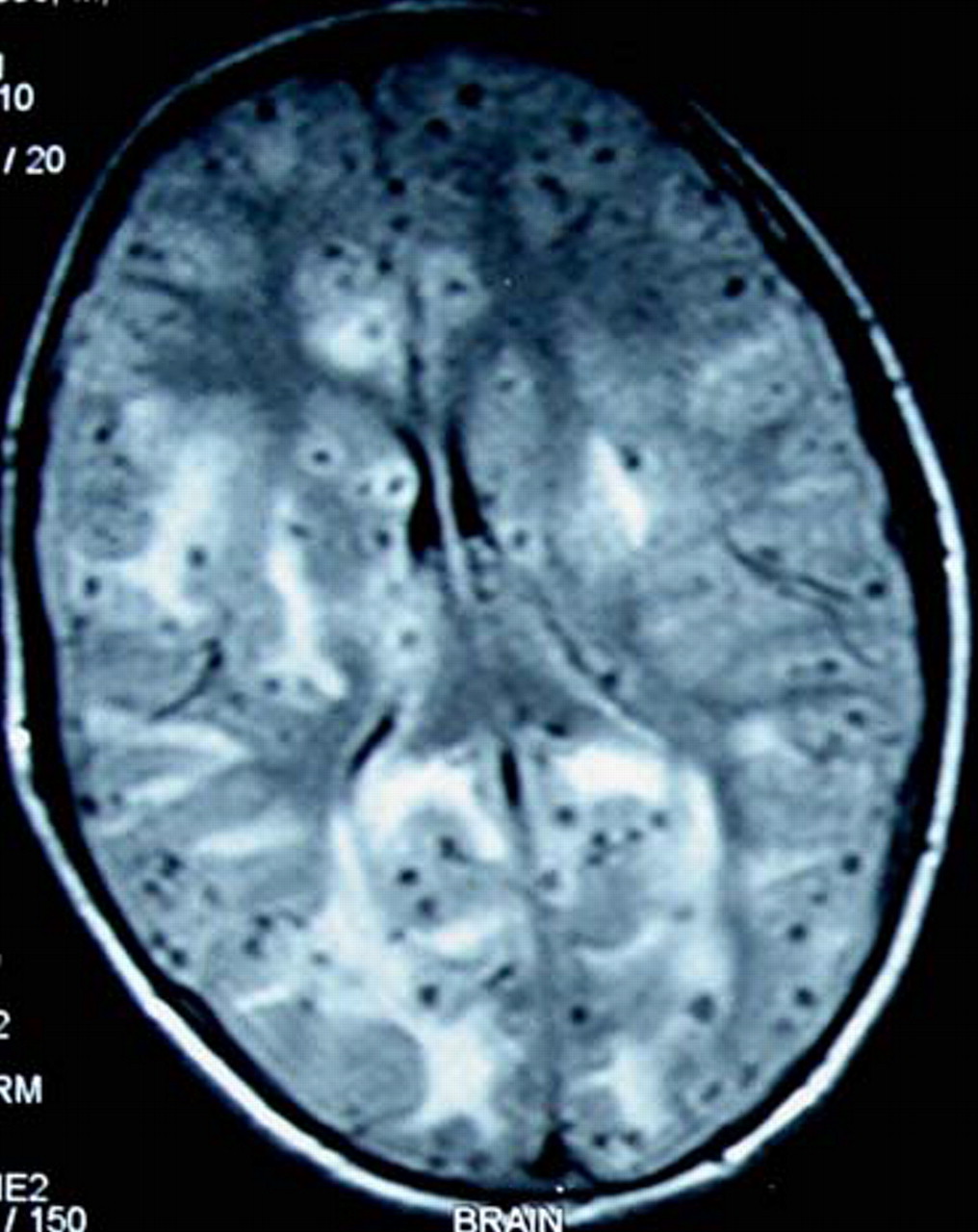
CT brain demonstrated diffuse cerebral oedema with multiple small cystic lesions scattered bilaterally (figure 1). MR images revealed innumerable well-defined small-sized cystic lesions (low signal on T1 and increased intensity on T2) and few, with tiny intralesional calcified, foci (typical appearance of scoleces) in the bilateral brain parenchyma with significant white matter oedema in the frontal regions (figures 2 and 3). These findings on the MR images were pathgnomonic of neurocysticercosis and resembled the picture of Swiss-cheese.
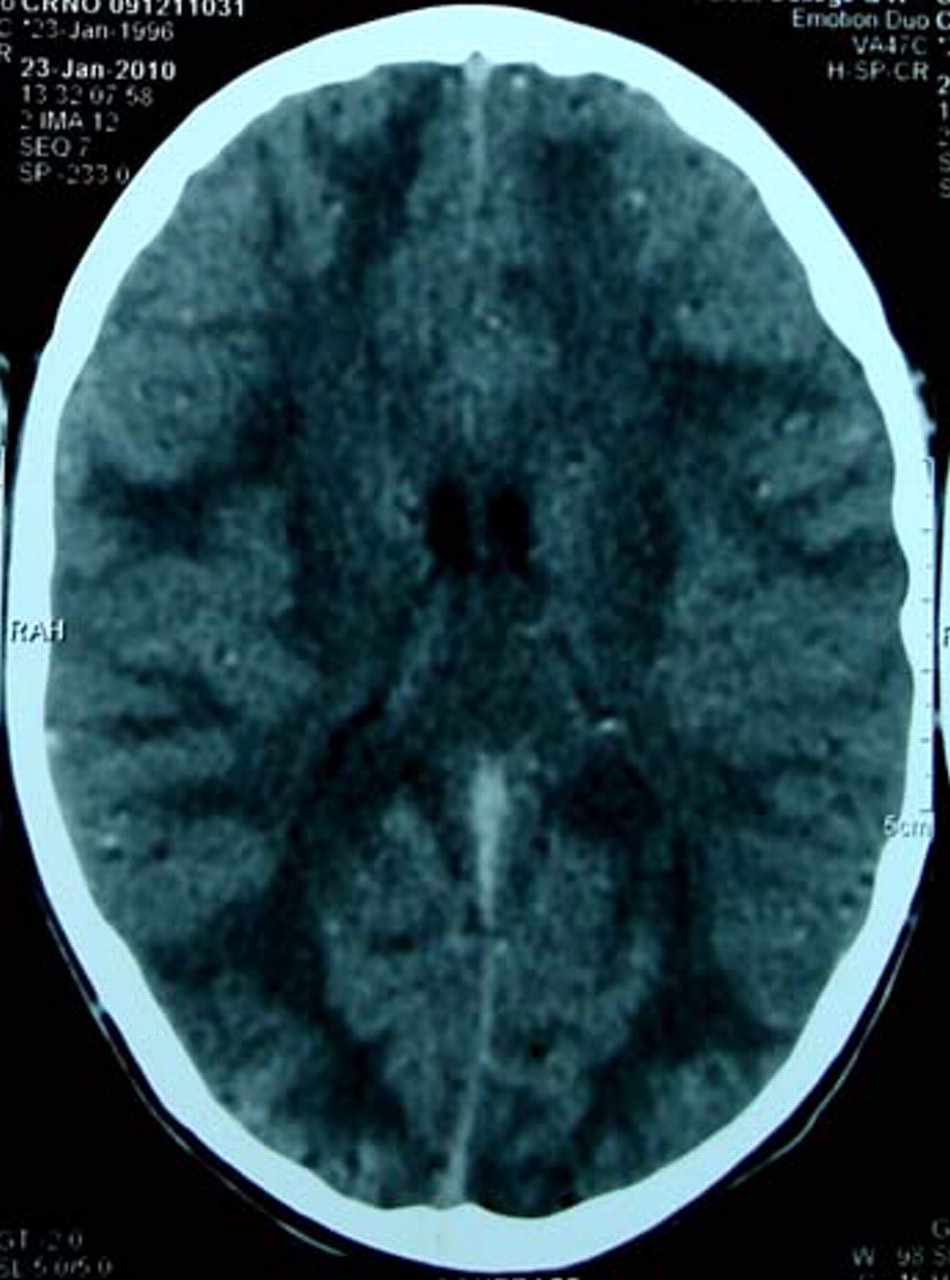
CT brain showing diffuse cerebral oedema with multiple small cystic lesions scattered bilaterally.

MR images with innumerable low-signal small-sized cystic lesions resembling Swiss-cheese.

{kind=link}
{kind=link}
{kind=link}
MRI brain showing multiple lesions with tiny intralesional calcified foci resembling starry sky.
Serum was positive for cysticercus immunoglobulin G antibodies by ELISA (1.60 optical density (OD) units; reference range, <0.9 OD units). There was no evidence of cysticerci in the thighs, subcutaneous tissues or the posterior segment of the eye. The patient was treated with intravenous antiepileptic drugs, glucocorticoids and antioedema measures. Subsequently after 48 h, the patient was started on albendazole 400 mg twice a day, which was continued for 21 days. Patient showed significant improvement and remained seizure-free during hospitalisation. A repeat CT brain done 1 week later showed a decrease in the cerebral oedema.
Neurocysticercosis is the most common parasitic disease of the central nervous system. Humans are the intermediate hosts of pork tape worm (Taenia solium). Cysticercosis is caused by ingesting the ova of the T solium through unhygienic vegetables or water. The diagnosis of cysticercosis is based on clinical, radiological and serological indicators. CT and MRI findings in parenchymal neurocysticercosis vary depending upon the stage of parasital development and the site of involvement, which may be parenchymal, intraventricular or meningobasal. Vesicular cysticerci appear as small, well-defined low-attenuation lesions (with eccentric hyperdense nodule interiorly representing the scolex) lacking perilesional oedema and enhancement after contrast medium administration. On MRI vesicular stage, scolex is usually visualised within the cyst as a high-intensity nodule giving the lesion a pathognomonic ‘hole-with-dot’ imaging and sometimes as in our case, these parasites are so numerous that the brain resembles a ‘Swiss-cheese’ or ‘starry sky’.1
Praziquantel and albendazole are the two antiparasitic drugs that have been reported to be effective against cerebral parenchymal cysticercosis lesions.2 However, albendazole is potentially more efficacious in treating the subarachnoid, ventricular and spinal cysts. In order to minimise the risks associated with the anticysticercal treatment (cerebral oedema, vasculitis), it is important to administer corticosteroids concomitantly, especially if there is high parasite load.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.