Article Text

Statistics from Altmetric.com
Description
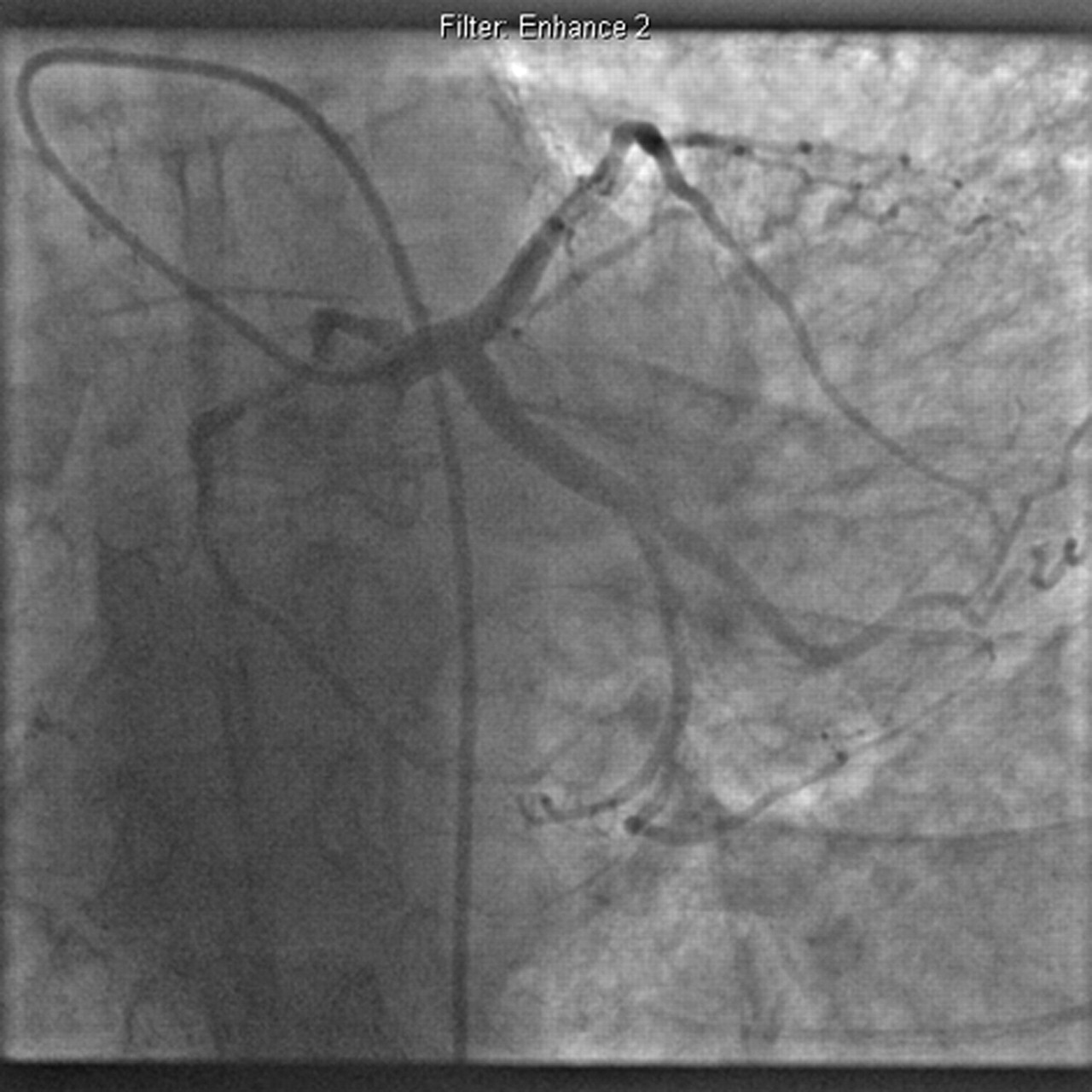
An old man with no cardiac history presented with breathlessness at rest and worsening exercise tolerance. Physical examination revealed an ejection systolic murmur and signs of left ventricular failure. The admission ECG showed voltage criteria for left ventricular hypertrophy with anterolateral repolarisation abnormalities. An urgent echocardiogram confirmed severe stenosis of a trileaflet aortic valve. Coronary angiography prior to aortic valve replacement demonstrated an anomalous dominant right coronary artery (RCA) originating from the left main stem but no atherosclerotic changes (figure 1).

Coronary angiography demonstrating an anomalous right coronary artery originating from the left main stem.
This finding is an extremely rare variant of the single coronary artery. The reported incidence of a single coronary system arising from the left sinus of Valsalva is 0.04%, with an RCA originating from the left main stem accounting for 0.65% of these.1 A multidetector CT scan confirmed the diagnosis (figure 2) and demonstrated an RCA course between the aorta and the main pulmonary trunk.

{kind=link}
{kind=link}
A multidetector CT scan demonstrating the anomalous right coronary artery originating from the left main stem.
This pathway can be associated with dynamic external compression by the great vessels causing angina pectoris, myocardial infarction, syncope and sudden death.2 However, in the absence of clinical or angiographic evidence of significant dynamic compression, the patient subsequently underwent aortic valve replacement without re-implantation of the right coronary artery. He unfortunately died 2 weeks later as a consequence of left ventricular hypertrophy and myocardial fibrosis resulting from severe aortic stenosis.
This case illustrates a rare anomaly. Nonetheless, it should be remembered that it can have clinically significant consequences, and it is therefore important to evaluate any dynamic external compression.
Footnotes
-
Competing interests None.
-
Patient consent Not obtained.