Article Text

Statistics from Altmetric.com
Description
The histologic sine qua non sought for a diagnosis of Wegener's granulomatosis (WG) are vasculitis, (geographic) necrosis and granulomas in the appropriate clinico serologic context.
That these pathognomons may be altogether absent, leading to misdiagnosis and mistreatment, should be remembered, as illustrated by this case.1
The patient was a 30-year-old woman beleaguered with intermittent cough and dyspnoea on exertion, and insignificant physical findings, at presentation, and nodulolinear, pulmonary infiltrates on imaging. Transbronchial lung biopsy, significantly, was bereft of necrosis, granulomas, neutrophlic microabscesses or vasculitis; instead depicting histology classic for BOOP (figure 1).
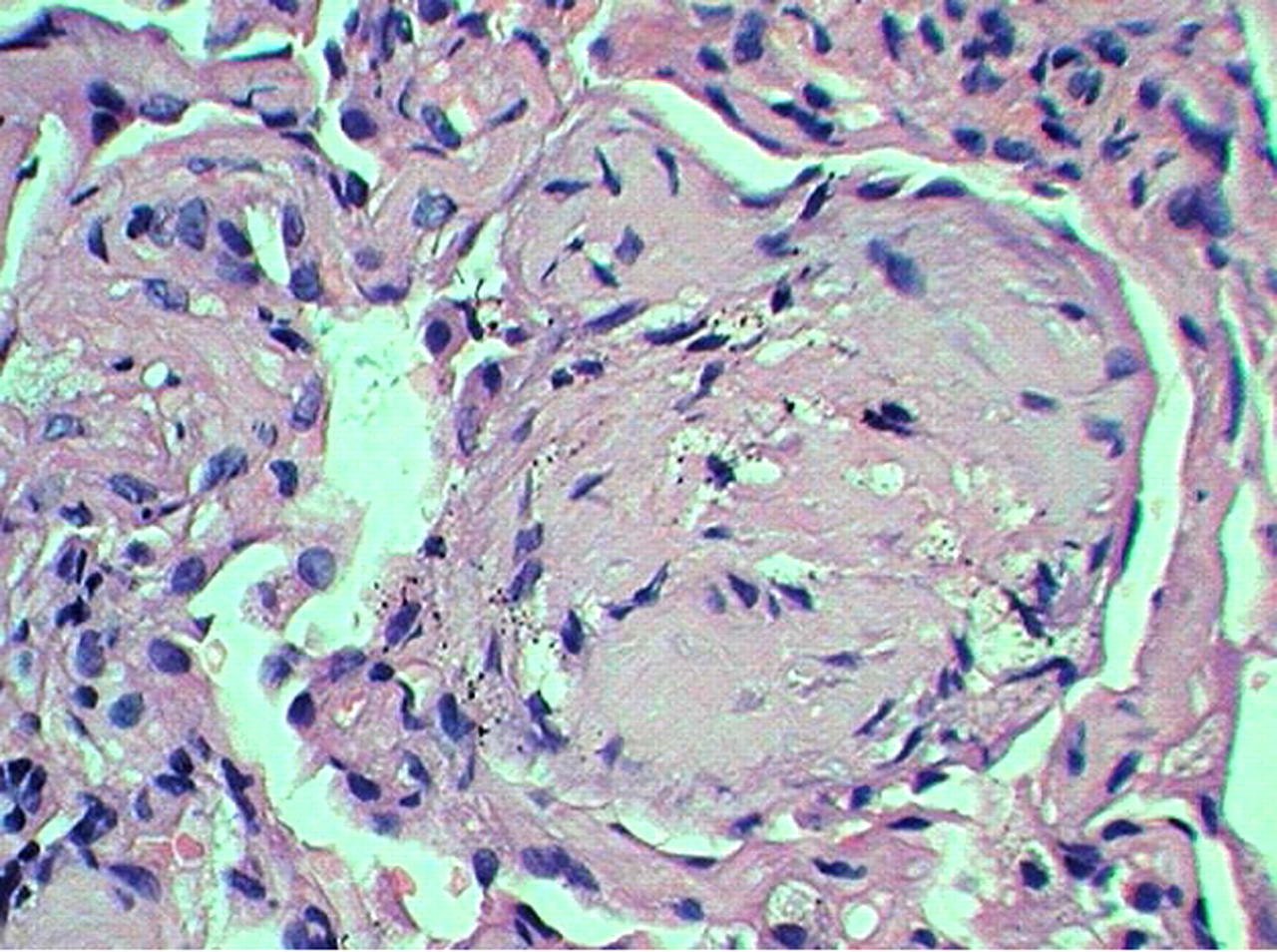
Transbronchial lung biopsy (H&E, ×40) fibrous plug occluding an alveolus (arrow), and a degree of fibrous interstitial expansion, diagnostic of BOOP. No necrotising vasculitis was discerned in the biopsy.
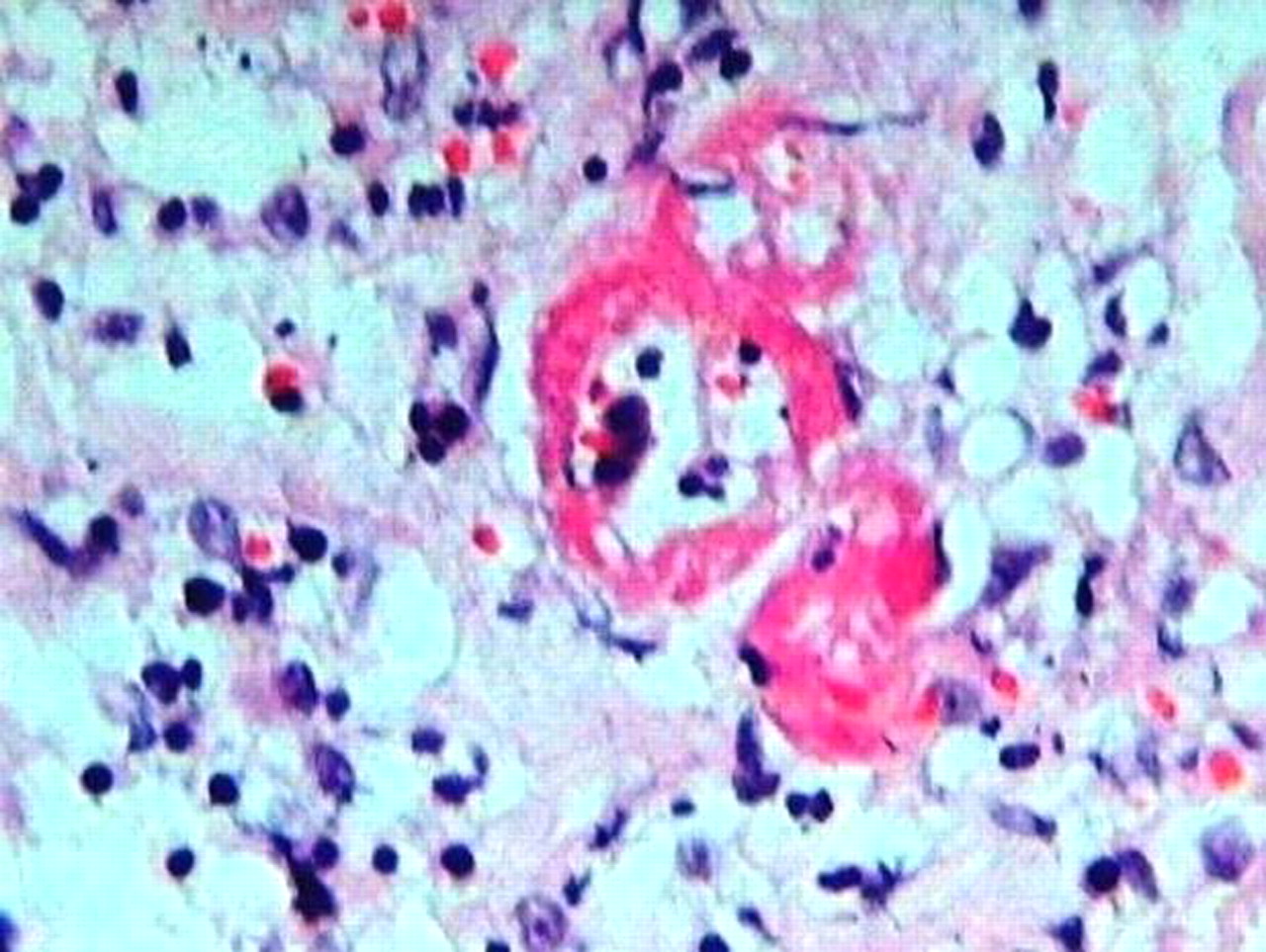
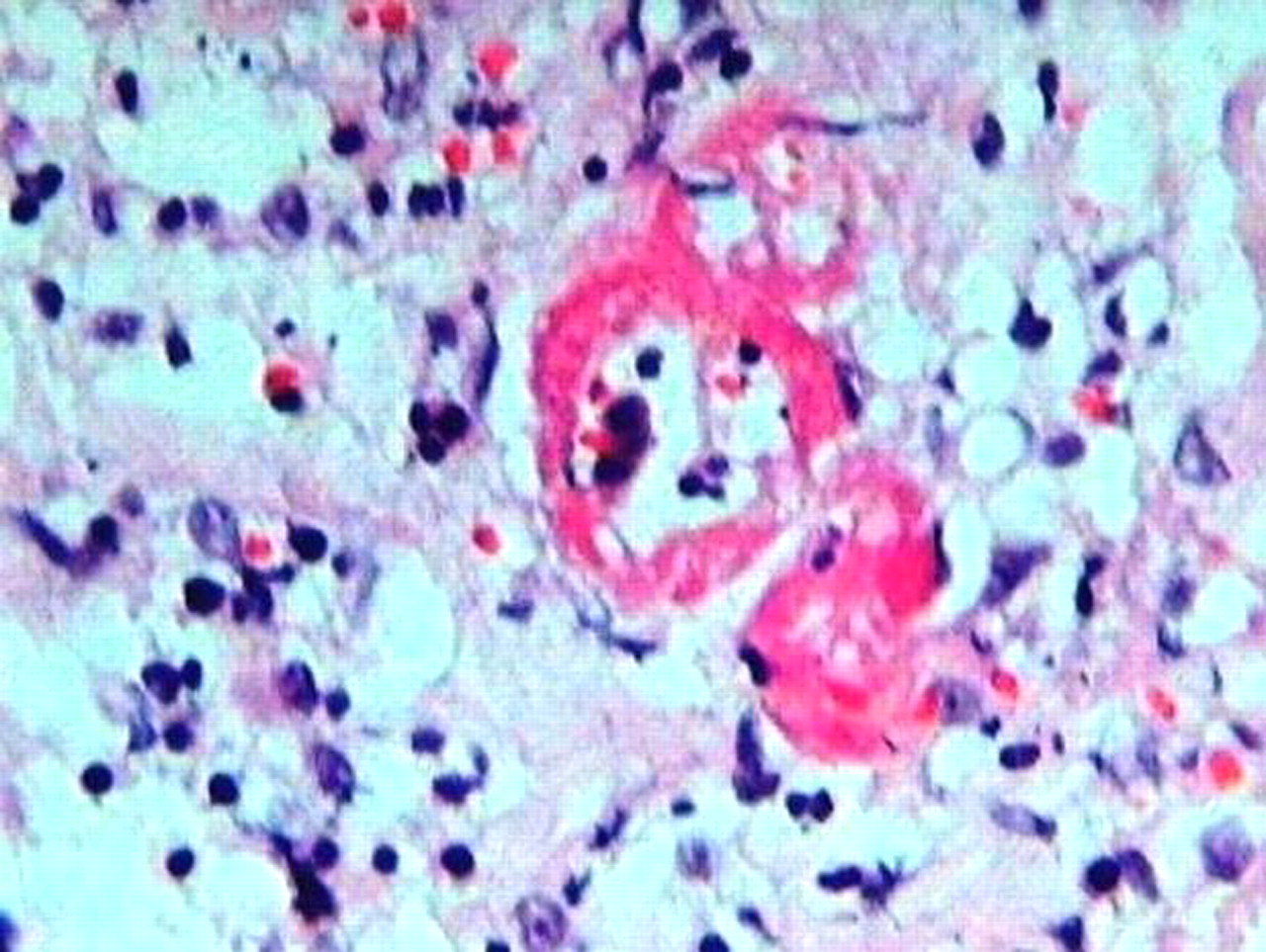
The patient was started on steroids, but remained clinically obdurate and developed stridor. Direct laryngoscopy revealed an excoriated mucosal lesion in the epiglottis; histology of which revealed active vasculitis, neutrophilic fragmentation and necrosis (figure 2). Immunofluorescent test for cytoplasmic antineutrophil cytoplasmic antibodies performed, based on histology, returned high positive and a diagnosis of Wegener's was made.
{kind=link}
{kind=link}
Larynx biopsy (H&E, ×40) necrotising vasculitis (arrow), neutrophilic fragmentation and oedema. Parenchymal necrosis and small granulomas were present elsewhere.
Travis et al (1991) describe the histologic manifestations of pulmonic Wegener's, dichotomised as major and minor. The three major pathologic manifestations of classical WG included parenchymal necrosis, vasculitis and granulomatous inflammation accompanied by an inflammatory infiltrate composed of a mixture of neutrophils, lymphocytes, plasma cells, histiocytes and eosinophils. The minor histologies included interstitial fibrosis, alveolar haemorrhage, tissue eosinophils, organising intraluminal fibrosis, endogenous lipoid pneumonia, lymphoid aggregates and a variety of bronchial/bronchiolar lesions including acute and chronic bronchiolitis, follicular bronchiolitis and bronchiolitis obliterans. They found the minor manifestations most commonly associated with classical WG lesions, and when the association was present – these were usually inconspicuous and not useful as primary diagnostic criteria. These authors found the minor lesions representing the dominant or major finding in a proportion of cases.2
It is this latter category that can be the most confounding at the instance of initial histologic assessment.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.