Article Text

Statistics from Altmetric.com
Description
A 26-year-old woman presented to our medical assessment unit with a 2-week history of breathlessness and cough. She was a lifelong non-smoker and had kept a parrot for many years. She was in type 1 respiratory failure with oxygen saturations of 87% and PO2 of 7.8 kpa breathing room air. A chest radiograph showed multiple nodules in a miliary pattern (figure 1). There was no evidence of consolidation. High resolution CT scan of thorax (figure 2) demonstrated extensive centrilobular ground glass opacities with no evidence of honeycombing. Serum avian precipitins (IgG antibodies) were significantly raised. There was no evidence of bacterial, viral or fungal infection on bronchoalveolar lavage fluid examination. Significant hypoxia precluded a trans-bronchial lung biopsy. The clinical and radiologic picture suggested the diagnosis of hypersensitivity pneumonitis (HP) secondary to avian exposure. Although chest radiograph may be normal in a majority of patients with HP1 and may rarely present as consolidation,2 this case suggests that miliary nodules on chest radiograph should raise the possibility of HP in appropriate clinical setting. The patient responded well to oral prednisone and withdrawal of exposure to antigen and a follow-up radiograph after 3 months showed significant resolution of the nodular change (figure 3). Differential diagnoses of miliary radiological pattern are protean and include miliary tuberculosis, primary or secondary pulmonary malignancy, sarcoidosis, pneumoconiosis or histoplasmosis. This case illustrates that HP should be considered in the differential diagnosis of miliary shadowing on chest radiograph.
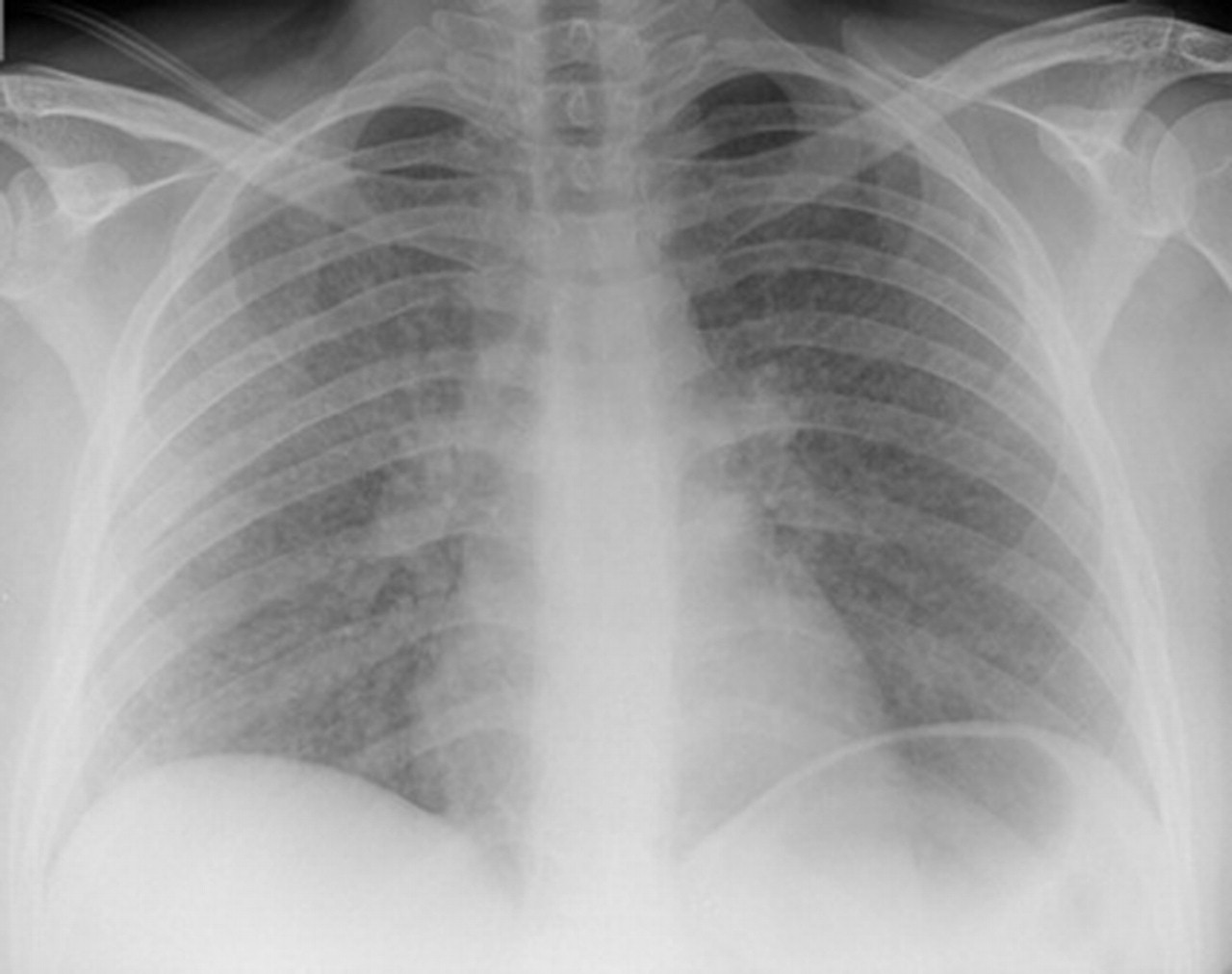
Extensive nodular shadowing on chest radiograph at presentation.

Thoracic high resolution CT scan demonstrating ground glass nodules in a predominantly centrilobular distribution suggestive of a radiological diagnosis of hypersensitivity pneumonitis.

{kind=link}
{kind=link}
{kind=link}
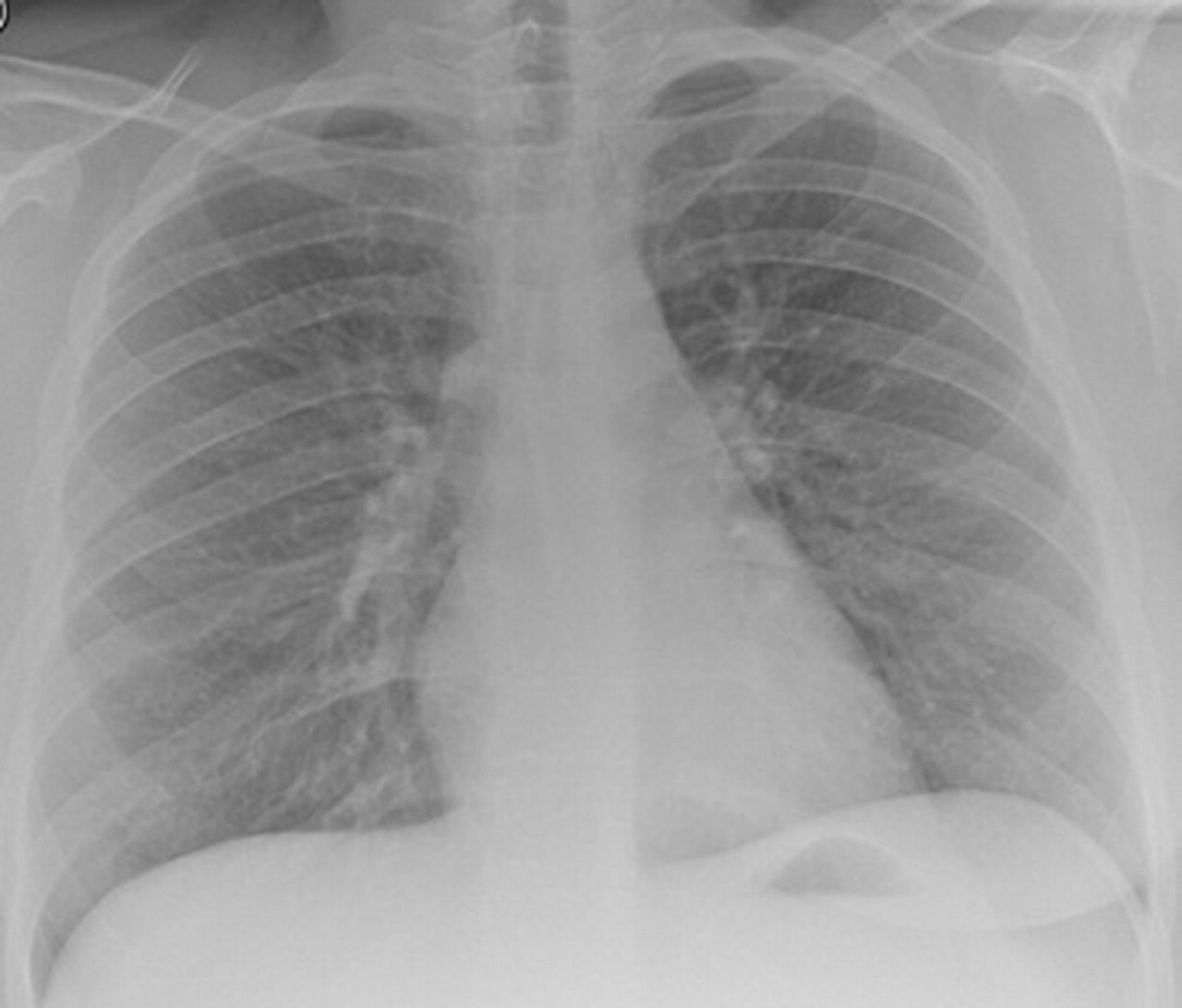
Follow-up chest radiograph following cessation of antigen exposure shows considerable resolution of nodular shadowing seen at presentation.
Acknowledgments
The authors thank Dr N Jagirdar for providing the radiological images for this case.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.