Article Text

Summary
The authors present a case of calcified posterior cruciate ligament (PCL). A 61-year-old female presented in our department reporting 12 months history of knee pain that was getting worse during the night. The patient was under medication for epileptic seizure, osteoporosis and hyperthyroidism. X-rays demonstrated calcification of the PCL. CT and MRI excluded any other intra-articular and extra-articular pathology. Arthroscopic debridement of the calcium deposits was performed and the symptoms resolved immediately, while the postoperative x-rays were normal. Histological examination confirmed the calcium nature of the lesion. Two years postoperatively the patient remains asymptomatic.
Statistics from Altmetric.com
Background
Knee ligaments calcification is a rare clinical entity. Pellgrini1 was the first to describe in 1905 ossification of medial collateral ligament (MCL) and Stieda2 in 1908 reported a case series of five patients. Fonda3 reported a case of calcified posterior cruciate ligament (PCL) along with osteochondritis dessicans of the lateral femoral condyle in 1955. No case of isolated PCL calcification has been reported in the literature so far. We report the clinical presentation, treatment and clinical outcome of our patient. Our patient was informed that data concerning the case would be submitted for publication.
Case presentation
A 61-year-old female presented at the accident and emergency department of our hospital, with right knee pain and decreased range of motion (ROM) following a fall. She reported right knee pain during the past 12 months without any history of trauma. The pain was non-specific and worsened during the night. She had no prior consultation for her symptoms up to her presentation but she used symptomatic treatment with painkillers. Her medical history revealed that she had been under medication for epileptic seizures (valproate), osteoporosis (alendronate, calcium and vitamin D) and hyperthyroidism (propylthiouracil). During physical examination, there was diffuse tenderness without any knee swelling. There was a lack of 30° of knee extension. No signs of meniscus pathology or instability were detected.
Investigations
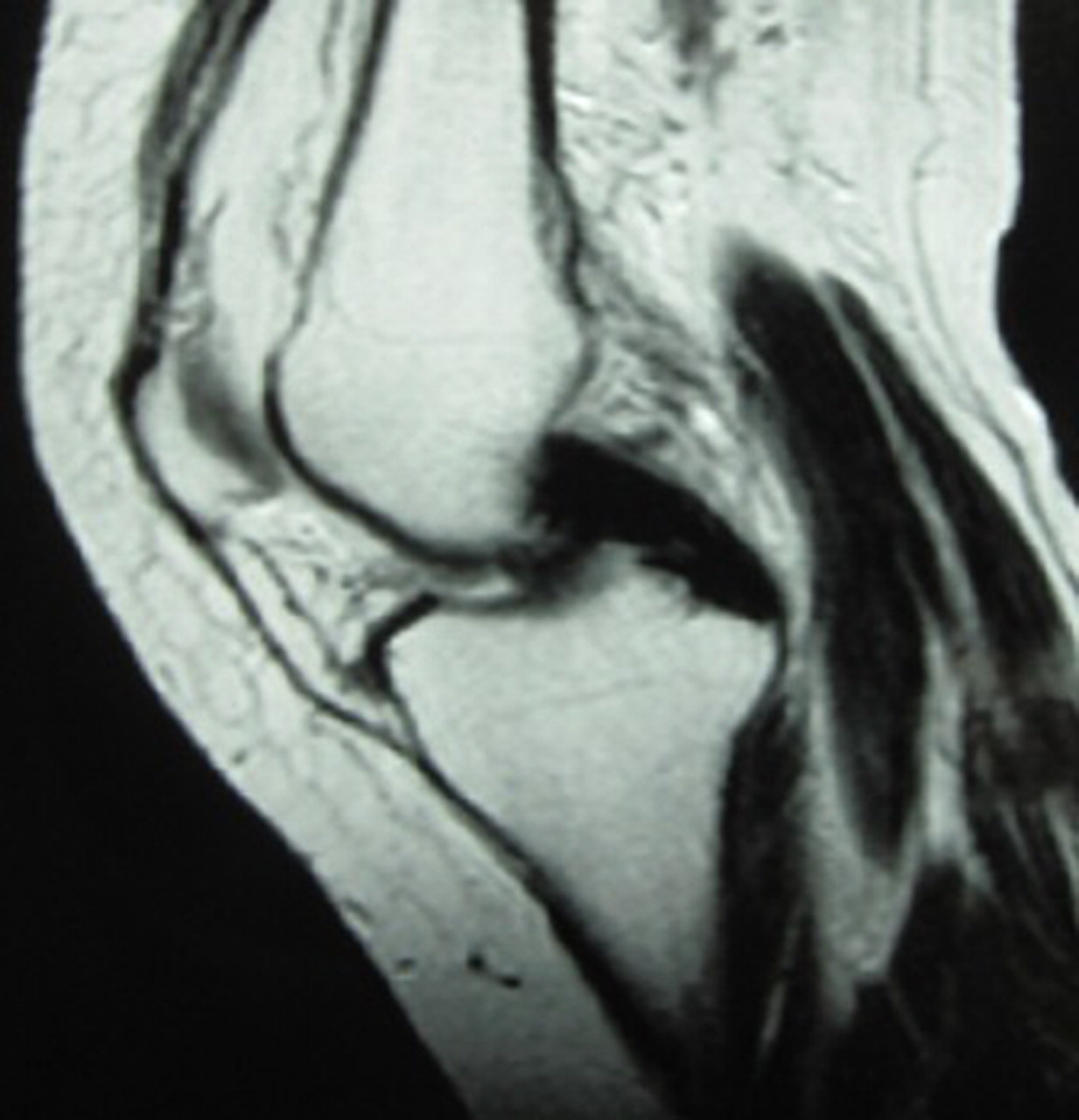
Anteroposterion, lateral and oblique radiographs demonstrated calcification of PCL (figure 1). Blood tests (haematological and biochemical) and hormonal control (T3, T4, thyroid stimulating hormone) were within normal values. CT and MRI of the knee were performed to exclude any intra-articular pathology that could cause the knee extension deficit. CT (figure 2) and MRI (figure 3) confirmed the calcification of the PCL and excluded any meniscal, chondral or other pathology that could result in ROM deficit.

Anteroposterior and lateral radiographs of calcified posterior cruciate ligament.

MR image of calcified posterior cruciate ligament.
CT (reconstruction) image of calcified posterior cruciate ligament.
Treatment
The patient was scheduled for arthroscopic debridement of the calcified PCL. Arthroscopic debridement of the synovium covering the PCL, through standard anterior and postero-medial portals (figure 4), released the calcium deposits, while no other pathology was found. A smooth shaver, the probe and small curettes were used to remove as much calcium deposits as possible without damaging the PCL fibres. The pathological tissue was sent for histological examination.
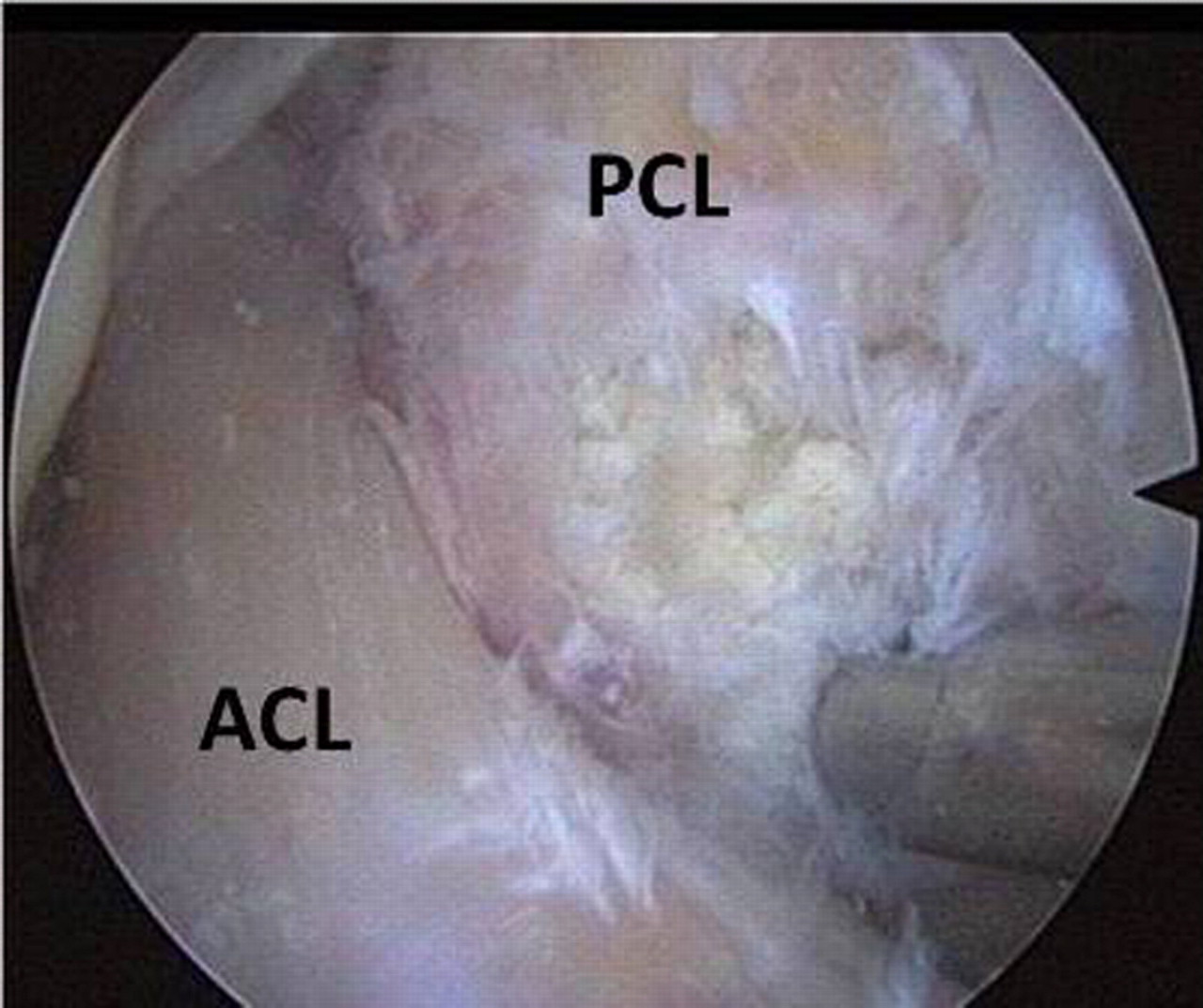
Arthroscopic view of the notch demonstrating the calcium deposits. ACL, anterior cruciate ligament; PCL, posterior cruciate ligament.
Outcome and follow-up
Postoperatively the patient was allowed full ROM and weight bearing as tolerated, using crutches. Postoperatively, the radiographs demonstrated that the PCL was clear of calcium deposits (figure 5) and the patient reported complete relief of her symptoms. Histological examination showed calcium deposits within the pathological tissue. The patient remains asymptomatic, 2 years after the operation with no signs of anteroposterior instability and normal x-rays.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Normal postoperative radiographs.
Discussion
This is the first case of isolated PCL calcification reported to our knowledge in the literature and as a result, the aetiology, clinical presentation, treatment and natural history are largely unknown. Pain is probably generated through the irritation of the nerve fibres of the synovium covering the PCL, by the calcium deposits that increase the pressure into the synovium. The diffuse character of pain could be explained by the localisation of the lesion. PCL is extra-synovial, intracapsular anatomic structure, surrounded by osseous and muscle tissue. Consequently, if the PCL is the origin of pain, the patient may not be able to specifically locate the pain.
MCL is a common site of ossification in the knee1,2 but with different clinical presentation. The ossification is originated by the femoral attachment of the MCL and is usually restricted there, without involving the whole ligament. Moreover, there is always a history of trauma that, in theory, results in hydroxyapatite or calcium pyrophosphate dyhydrate crystal deposition.4
Interestingly, similar clinical presentation to our case has been reported by Tsujii et al5 in a case of calcified anterior cruciate ligament. Pain and restriction of knee motion were the predominant symptoms that resolved immediately after arthroscopic excision of the synovial membrane. The main difference of the case of Tsujii et al5 compared to our case is the history of a knee twisting injury that caused the onset of symptoms.
In our case of PCL calcification, there is no history of trauma and as a result, we should look for a different aetiology. Several diseases have been reported as predisposing factors or possible causes of calcified supraspinatus. Calcium deposits have been associated with thyroid disorders, diabetes, hyperparathyroidism, hypervitaminosis D and oestrogen metabolism.6 Our patient was under medication for epileptic seizure (valproate), osteoporosis (alendronate, calcium and vitamin D) and hyperthyroidism (propylthiouracil). It is known that thyroxine is important for both collagen synthesis and matrix metabolism. Moreover, in women after menopause oestrogens are known to have wide-ranging effects on connective tissue metabolism. The metabolic pathway that could possibly lead to PCL calcification cannot be determined in our case and has not been recognised in shoulder calcific tendonitis either. What is known in our case, is that at the time of admission, our patient’s blood and hormonal tests were within normal values. Nevertheless, we are not aware of the patient’s hormonal profile during the onset of the symptoms, 1 year ago.
Arthroscopic treatment and debridement of the calcium deposits through standard anterior and postero-medial portals proved efficient in our case. The release of the pressure of synovium nerve fibres potentially explains the pain relief. Debridement of the lesion has been used in rotator cuff tendons calcification with good clinical results.7 Complete removal of the lesion is not considered to be necessary. In our case, the calcific deposits were partially removed and special care was taken not to compromise the integrity and competence of the PCL. In our opinion, debridement of the synovium makes possible the calcium remnants diffusion into the joint and consequently their absorption. Whether debridement of the synovium covering the posterior surface of the PCL, through the postero-medial portal, is mandatory or not, cannot be determined. The reason we used both anterior and posterior portals was to ensure as much calcium deposits removal as possible.
Learning points
▶ Isolated PCL calcification is a new clinical entity of unknown aetiology.
▶ The main symptom of calcified PCL is diffuse knee pain.
▶ Arthroscopic debridement of the calcium deposits seems to be effective.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.