Article Text

Statistics from Altmetric.com
Description
A 22-year-old male presented with complaints of bilateral flank pain along with nausea and vomiting since 2 weeks. There was anuria since 2 days. Routine blood investigations revealed deranged renal function tests, blood urea was 132.7 mg% and serum creatinine was.14.7 mg%. Serum electrolytes, electrocardiogram (ECG) and arterial blood gas (ABG) levels were within normal range. Ultrasonogram showed bilateral renal and ureteric stones with moderate hydronephrosis. Plain skiagram kidney, ureter, bladder (KUB) revealed multiple right renal and ureteric stones; there was a solitary left renal stone and two stones in left lower ureter (figure 1).

Plain skiagram KUB region. Multiple right renal and ureteric stones, solitary left renal stone and two stones in left lower ureter.
Ultrasonography-guided bilateral per cutaneous nephrostomies were inserted under local anaesthesia (figure 2). Subsequent urine output was 1500–2000 ml on both sides. Appropriate fluid replacements were made and miraculously serum creatinine came down to 1.7 mg% after just 1 week of diversion.

Plain skiagram KUB region after bilateral per cutaneous nephrostomies.
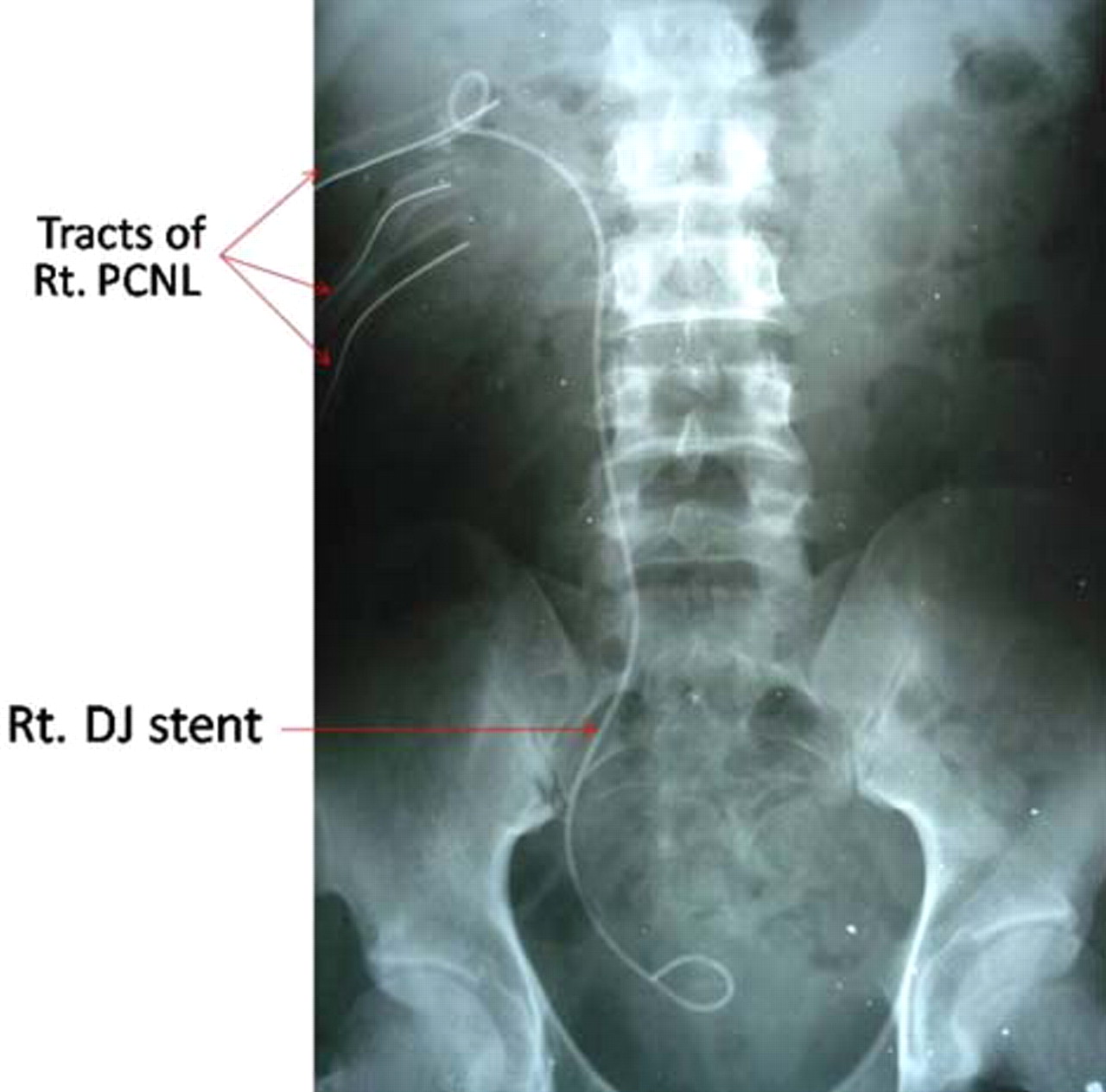
After stabilisation, the patient was subjected to endoscopic removal of stones. We used a semirigid ureteroscope and a rigid nephroscope. In one sitting, right ureterorenoscopy (URS) was done followed by left URS and left percutaneous nephrolithotomy (PCNL) achieving complete clearance of both ureters and left kidney (figure 3). After 3 days, we performed right PCNL and removed left double J (DJ) stent. Prior to this a right nephrostomogram was done (figure 4). All stones in the right kidney were removed employing three punctures and right DJ stent was kept (figure 5). No blood transfusions were needed. Patient was discharged after 3 days of second procedure and right DJ stent was removed after 3 weeks. The serum creatinine at the time of discharge was 1.31 mg% and all punctures had completely healed (figure 6).

Plain skiagram KUB region after bilateral URS and left PCNL. Complete clearance of ureteric stones and left renal stone. Bilateral DJ stents seen.

Right nephrostomogram delineating the pelvicalyceal anatomy and ureter.

Plain skiagram KUB region after right PCNL. Complete clearance of right renal stones. Right DJ stent seen.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Various puncture sites completely healed.
Discussion
On presentation, the renal functions showed gross derangements. However, since serum electrolytes, ECG and ABG values were normal and the patient did not have any respiratory symptoms, we did not subject the patient to dialysis. In a patient of obstructive uropathy, timely decompression may result in complete recovery of renal function.1 Decision to dialyse should not be undertaken on the basis of elevated serum creatinine alone; in this patient serum creatinine was 14.7 mg% at presentation and no dialysis was needed. Rather dialysis should be offered to patients presenting with refractory hyperkalaemia or hypervolaemia, ECG changes, uremic encephalopathy and respiratory decompensation.
In the past, large incisions were needed to extract urinary tract stones. With the advent of endourology, stones anywhere in the urinary tract may be managed in a minimally invasive fashion.
The right kidney harboured multiple stones in all the calyces. Since we were using a rigid nephroscope, we had to make multiple punctures (upper, middle and lower calyces). Employing a flexible nephroscope could have decreased the number of renal punctures but would have increased the operative costs.2 PCNL, if correctly performed, results in minimal blood loss. In this patient, a total of four renal punctures were made (one on the left and three on the right) without the need for any blood transfusions.
Endourology is the gold standard for managing urolithiasis.3 No or very small incisions are made that reduces blood loss, avoids patient disfigurement and cuts down on the hospital stay and cost. As the procedures are carried under fluoroscopy, it ensures maximal stone clearance, which is so relevant in a patient like this.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.