Article Text

Summary
The authors present two patients referred by colleagues after traumatic hand injury. However, upon closer inspection, both patients had pigmented lesions under the nail bed, which upon biopsy showed proven subungual malignant melanoma. The authors wish to emphasise the importance of this diagnosis, especially in emergency care.
Statistics from Altmetric.com
Background
We present two cases of subungual malignant melanoma, both presenting following trauma. The cases had been managed for long periods of time under the care of non-skin cancer specialists. Early detection in malignant melanoma is vital for improved treatment outcomes and prognosis. Subungual melanoma presents in a more disguised manner than cutaneous lesions and therefore requires increased vigilance and awareness.1 Both of our cases highlight how any pigmented lesions within the nail bed matrix should raise suspicion and the need for early referral and biopsy.
Case presentation
Patient 1 is a 68-year-old right hand dominant male, in previous good health, who presented 8 months following a crush injury to his right ring finger. He had been treated with oral antibiotics twice for cellulitis and was referred to plastic surgeons by his orthopaedic colleagues. Subsequently, a hyperpigmented nail bed was noted (figure 1), and though the patient was aware of it, he did not seek a specialist opinion. Punch biopsy confirmed subungual melanoma, with later excision showing invasive ulcerated subungal melanoma of Breslow thickness 1.37 mm with proximal nail fold extension with an acral lentiginous in situ component. He underwent an amputation of his right ring finger through the middle phalynx. Sentinel node of the axilla was negative, but supratrochlear nodes were positive, therefore supratrochlear clearance was carried out. Staging CT showed no evidence of metastatic spread in this case.

Hyperpigmented nail bed with loss of nail, right ring finger.
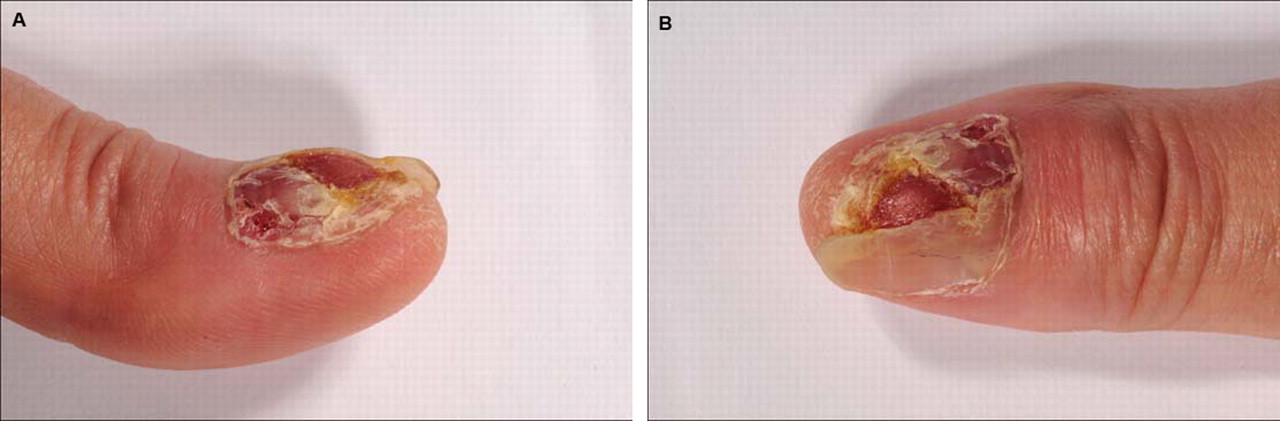
Patient 2 is a 59-year-old right hand dominant female who sustained an injury to her left thumb with a kitchen knife while preparing vegetables. The patient re-presented 2 years after the initial injury as her general practitioner was concerned about a small red tissue defect that was still draining (figure 2). The tissue defect and the nail were not healing and referral to orthopaedic colleagues and later plastic surgeons was sought. The main differential diagnosis at the time was believed to be a small pyogenic granuloma. A 3 mm punch biopsy was taken of an irregular pigmented lesion in the nail bed. Histology was reported as ulcerated invasive subungual melanoma with a Breslow thickness >2.5 mm. She underwent amputation of the left thumb with sentinel node biopsy. The nodes removed were reported as negative for metastatic melanoma. Both of our patients continue to have routine surveillance by the specialist skin cancer team.
{kind=link}
{kind=link}
Healing injury of left thumb with subsequent nail destruction and visible red nodule.
Discussion
Subungual melanoma is a rare type of skin cancer. It accounts for 23% of melanomas in the Japanese population, 25% in the Afro-Caribbean population and 1–3% in the White population.1 Overall, 62% of lesions present on the fingernails with 38% presenting in toe nails.2 Diagnosis is often delayed in those with subungual melanoma with patients going on to have a poorer prognosis than those with cutaneous melanoma. Similar clinical presentations include subungual haematoma and pyogenic granuloma.3 Estimated 5-year survival is between 16% and 87%.4 Histological diagnosis is the most definitive way of identifying such a lesion and can prevent significant morbidity and mortality. Both of these incidental cases are patients referred from specialties other than dermatology and plastic surgery, where skin cancer composes a larger proportion of the workload. Suspicious signs to be aware of are nail fold pigmentation (Hutchinson's sign), lifting off of the nail from the nail bed and ulcerating lesions that do not heal.5 Unexpected bone destruction on x-ray after hand trauma has led to documented cases in the accident and emergency department.5 A very useful approach is the ‘ABC’ rule for the clinical detection of subungual melanoma.4
A = Age (5–7th) decade Africans, Asians, Native Americans.
B = Brown to black discolouration, breadth of nail pigmentation >3 mm.
C = Change in nail band. Failure of nail dystrophy to improve despite adequate treatment.
D = Digit involved. This refers to the understanding that the thumb is most affected, followed by the hallux, any single digit and then finally multiple digits.
E = Extension of pigment to involve proximal or lateral nail fold (Hutchinson's sign).
F = Family or personal history of dysplastic nevus or melanoma.
This can be applied in a similar fashion to the ‘ABC’ approach detecting cutaneous melanoma, which has led to early identification. Each alphabet is not used in isolation, but with all letters together to improve early detection and survival of subungual melanoma.2 Prognosis depends heavily upon the thickness of the tumour, termed the Breslow thickness, the stage of the tumour and the degree of tumour invasion. Breslow thickness is known to be a good prognostic indicator for subungual melanoma, even though it is less accurate than that for cutaneous melanoma. Breslow thickness gives useful prognostic information, but does not give an indication of the extent of spread or the degree of nodal involvement. Nail apparatus can be thickened extensively invalidating prognostic accuracy.1 Up to 25% of patients can present with lymph node or distant metastases.3 It has been suggested that the diagnostic delay for subungual melanoma can be as great as 30 months.4 It is also believed that traumatic injury may be the initial cause for developing subungual melanoma.5 In both of our cases, we are unsure of whether trauma is the cause of the subungual melanoma, or whether the injury brought a pre-existing lesion to light. Nevertheless, our take home message is that an unresolving subungual lesion of any kind should raise a suspicion until proven otherwise and warrant early referral to a skin cancer specialist unit. A biopsy of the lesion is warranted as soon as possible along with a thorough clinical examination of regional and distant lymph nodes.
Learning points
▶ Unresolving subungual lesion of any kind should raise a suspicion until proven otherwise and warrant early referral to a skin cancer specialist unit.
▶ Biopsy of the lesion is warranted as soon as possible.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.