Article Text

Statistics from Altmetric.com
Description
Disseminated fungal sepsis in an extremely premature neonate. An infant born at 25 weeks gestation was extubated to biphasic continuous positive airway pressure after 7 days. On day 8, she developed a periumbilical rash from which Candida was isolated. Topical miconazole and intravenous antibiotics were started in view of increased desaturations and thrombocytopenia. On day 11, Candida albicans was isolated from blood cultures and intravenous fluconazole was commenced. Cranial and renal ultrasound scans were normal. She became progressively more unwell, needing ventilation. On day 14, she developed pulmonary haemorrhage. A cranial ultrasound scan showed several widespread circular echogenic lesions consistent with invasive fungal mycomas (figure 1).1
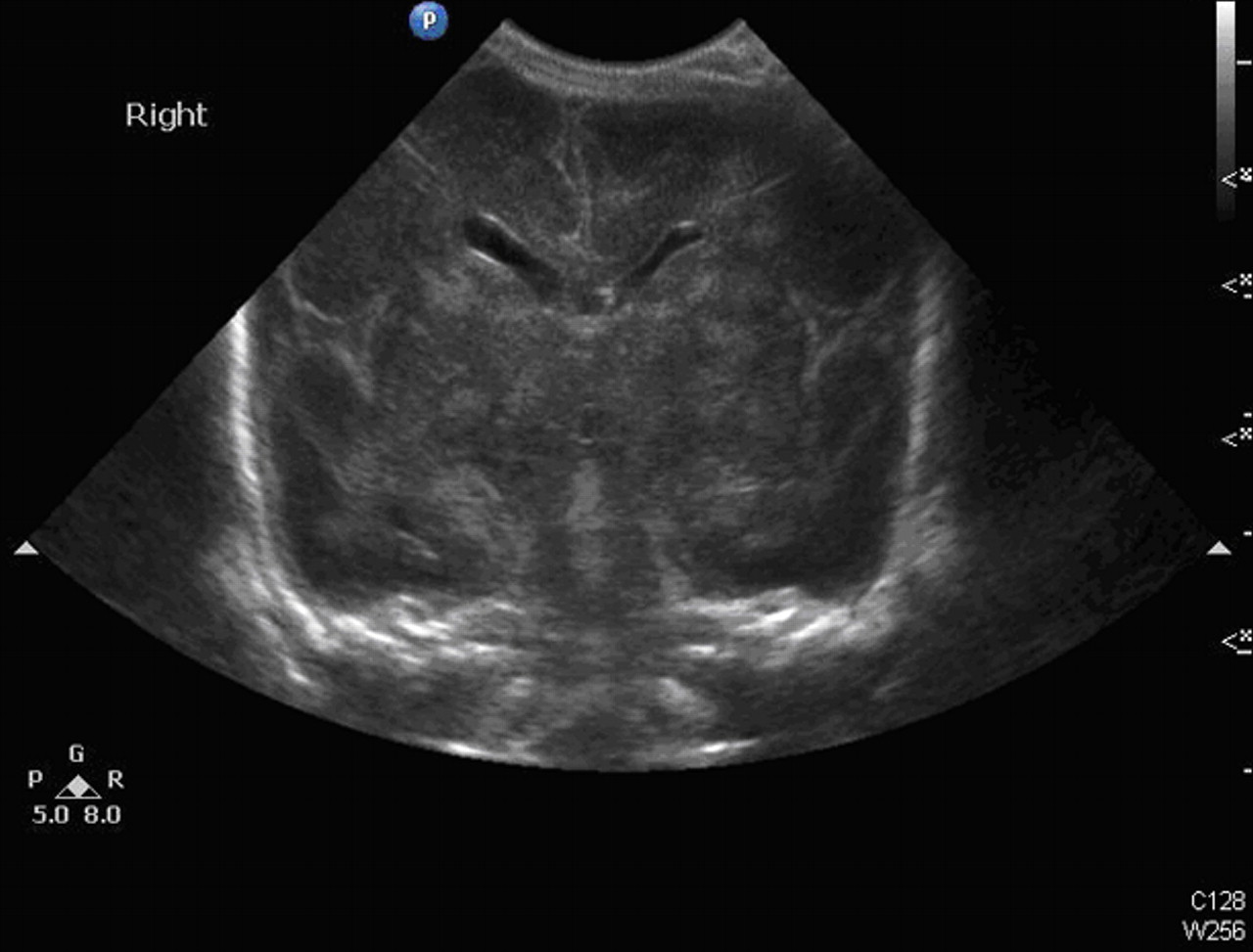
Bilateral widespread multiple spherical areas of increased echogenicity within the periventricular white matter and basal ganglia.
Although fluconazole provides good cerebrospinal fluid penetration, intravenous micafungin was added as broad spectrum antifungal therapy to provide cover for other strains of Candida in view of the clinical deterioration. Despite this, she became more unwell and intensive care was withdrawn.
Postmortem confirmed mycotic encephalitis (figure 2) with disseminated fungal sepsis within the liver, lungs and kidneys.

{kind=link}
{kind=link}
Multiple Candida granulomas within brain substance identified by grocott stain.
Acknowledgments
The authors would like to thank Perinatal Pathology Department, Birmingham Women's Hospital.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.