Article Text

Summary
In the emergency setting, shortness of breath is a frequent presenting complaint to physicians worldwide. The differential diagnosis is often broad and requires careful analysis of investigations to reach the correct diagnosis. The authors present a case of acute heart failure with a number of unusual presenting features that suggested an uncommon aetiology.
Statistics from Altmetric.com
Background
Acute heart failure is a common problem facing doctors in acute medical care. Usually occurring in patients with pre-existing heart failure, valvular disease or who present with acute coronary syndromes or tachyarrhythmias.1 Over the last four decades, the management of the acutely breathless patient with heart failure has altered little. The standard use of oxygen, loop diuretics, opiates and nitrates relieves symptoms for most within a few hours. Familiarity can sometimes lead to complacency and some patients do not respond well to conventional treatment. We present a rare case of acute heart failure, which was refractory to standard treatment requiring urgent echocardiography to appropriately diagnose and tailor management.
Case presentation
A 50-year-old man presented to our hospital's emergency department with a 3-day history of worsening dyspnoea. He denied experiencing angina, palpitations or syncope. He had no significant co-morbidities. Three months earlier he had ruptured his left Achilles tendon while playing football. This was treated with 10 weeks of below knee immobilisation and had been removed 3 weeks earlier. Preceding admission he had been otherwise well with no exertional limitation and was a keen medium-distance runner. There was no family history of inherited cardiac disease.
On clinical examination he was sweaty, tachypnoeic and hypoxic, his pulse was regular and measured 52/min and blood pressure was 106/60. His respiratory rate was 30/min. Auscultation of the chest revealed bilateral wheeze and basal crepitations. Heart sounds were normal and an ejection systolic murmur of varying intensity was audible and heard loudest at the left sternal edge and apex.
Investigations
Arterial blood gases on 15 litres/min of supplemental oxygen showed type I respiratory failure with a compensated metabolic acidosis (PaO2=9.3 kPa, PaCO2=4.0 kPa, bicarbonate=21.1 mmol/l, Base excess −4.8 mmol/l and pH=7.4).
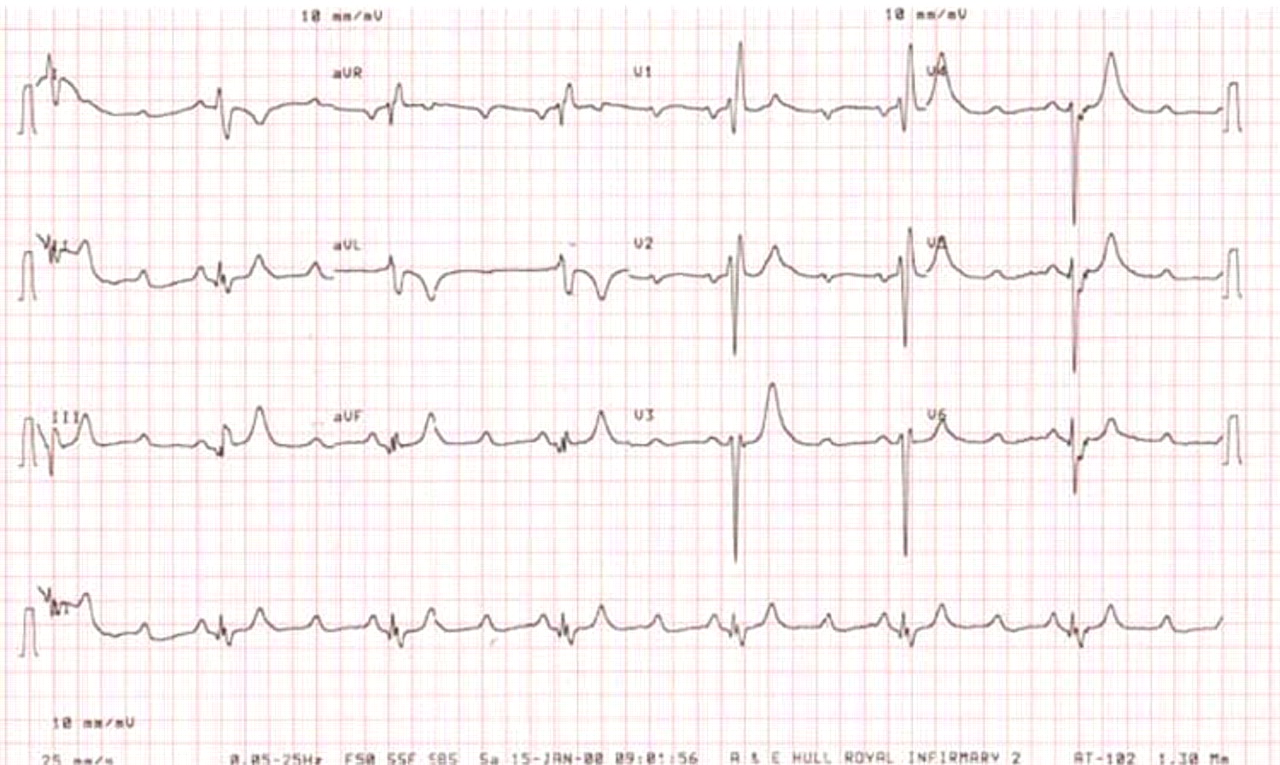
Initial ECG showed a heart rate of 42 bpm with right bundle branch block morphology and 3:1 second degree atrioventricular (AV) block, which intermittently reverted to a sinus bradycardia (figure 1).

12 Lead electrocardiograph at acute presentation showing 3:1 second degree atrioventricular block.
Chest x-ray confirmed the presence of pulmonary oedema.
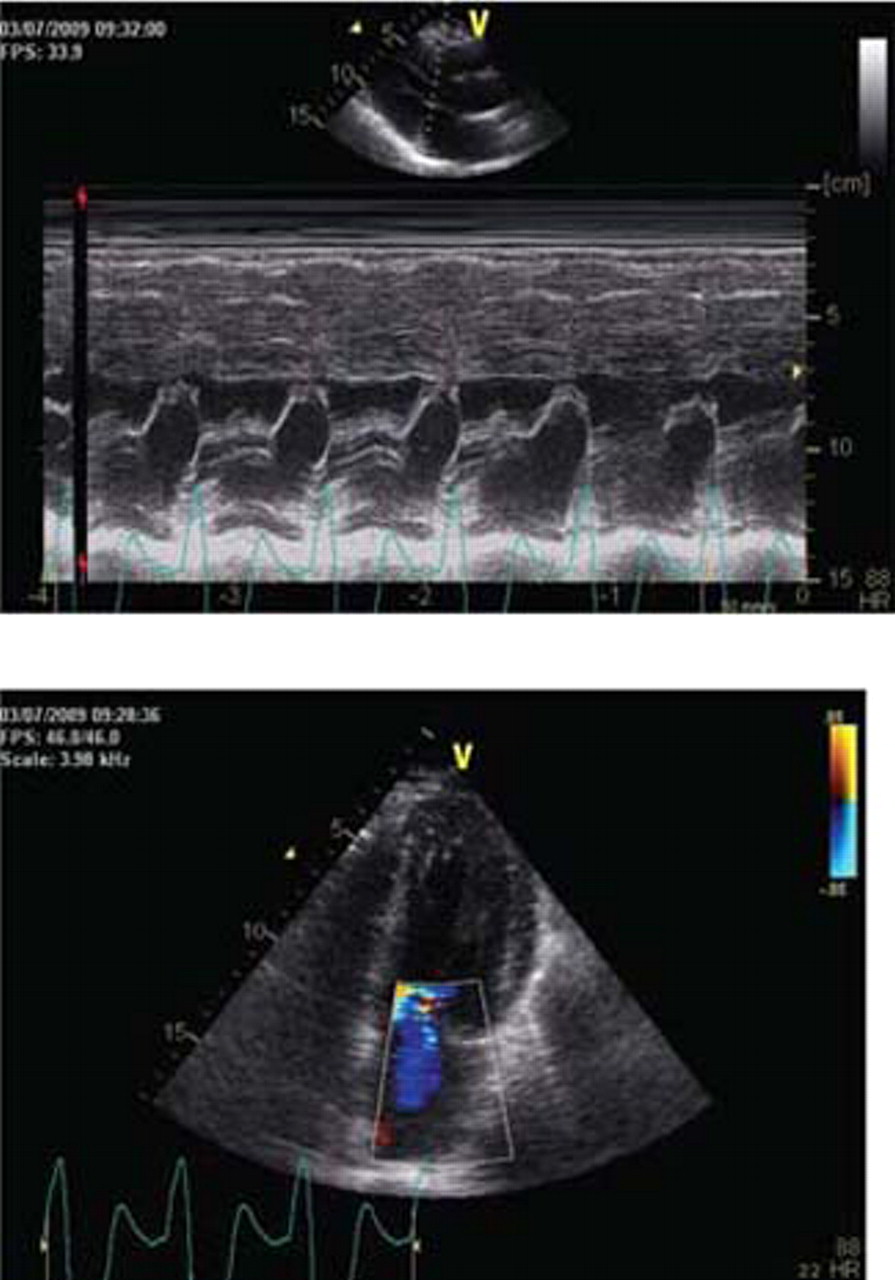
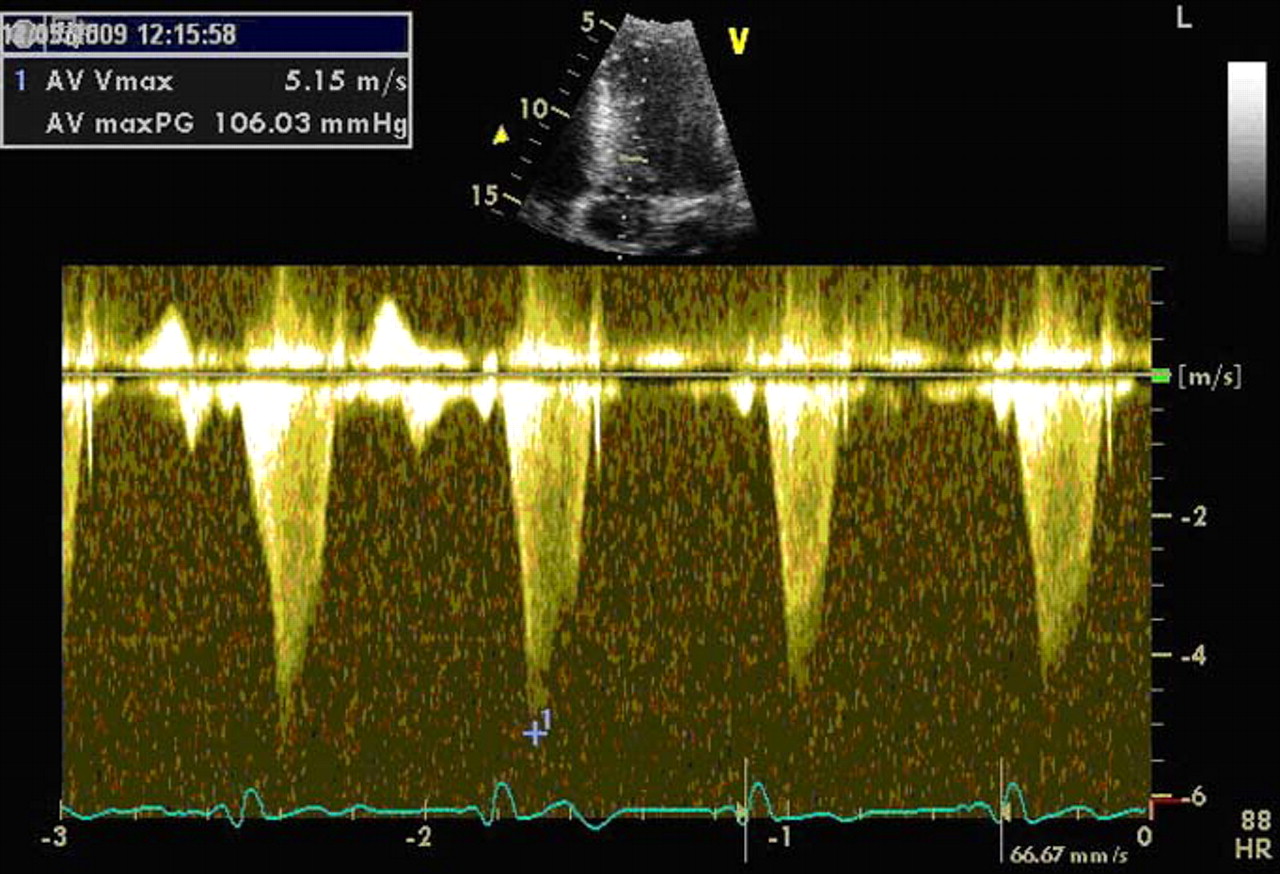
Urgent trans-thoracic echocardiogram performed during AV block showed good left ventricular (LV) contractility, hypertrophy of the anterior and septal LV walls (1.6 cm at end diastole), systolic anterior motion (SAM) of the mitral valve (figure 2), class IV mitral regurgitation (figure 3) and a dynamic LV outflow tract (LVOT) gradient with the peak velocity measuring 5.15 m/s (Peak gradient =106 mm Hg) (figure 4) There was no right ventricular (RV) dilation or measurable tricuspid regurgitation. No vegetations were seen.

M-mode Doppler showing classical systolic anterior motion of the mitral valve prior to right ventricular pacing.

Colour Doppler showing severe class interventricular mitral regurgitation.

Continuous wave Doppler through the left ventricular outflow tract showing a severe gradient with classical dagger shaped contour.
CT pulmonary angiogram showed no thrombus within the pulmonary vasculature.
Troponin T level was elevated at 0.21 mcg/l.
Differential diagnosis
The differential diagnosis is broad but, given the combination of pulmonary congestion coupled with ECG changes, it would suggest this is primarily a cardiac cause. The differentials were acute heart failure secondary to LV systolic impairment or valvular disease (de novo or acute on chronic), bacterial endocarditis, sepsis, vasculitis or pulmonary embolism.
Treatment
Standard treatment consisting of intravenous morphine and diuretics was given initially but the underlying aetiology of his presentation remained unclear. After transfer to the coronary care unit, it was observed that episodes of pulmonary oedema with marked dyspnoea coincided with a change in cardiac rhythm from sinus to second degree AV block. A temporary pacing wire was inserted and he was paced from the RV apex. Over the next 24 h there was marked clinical improvement. Temporary pacing significantly reduced the severity of mitral regurgitation, SAM and outflow tract obstruction. Coronary angiography showed normal coronary arteries. On day 3 of his admission, a dual-chamber rate adaptive pacemaker was implanted with a short programmed AV delay and he was started on β blockers.
Outcome and follow-up
By 6–weeks’ follow-up, he had complete resolution of symptoms and returned to his normal level of activity.
To rule out Fabry's disease we tested the level of α galactosidase and this was within the normal range. During maximal cardiorespiratory exercise testing using modified Bruce protocol he exercised for 14 min 37 s. His heart rate response was blunted but blood pressure response normal. The peak VO2 was lower than predicted (21 ml/kg/min, respiratory exchange ratio at peak exercise=1.08) and Ve/VCO2 slope elevated at 33 ml/kg/ min. Recumbent bicycle ergometry was performed using a ramp protocol. His resting LVOT peak velocity was now 1.9 m/s (14.4 mm Hg) (figure 5). He attained stage IV of the protocol. There was a marginal increase in the LVOT velocity to 2.2 m/s at maximal exertion. Only trivial mitral regurgitation was seen at rest and at peak exertion and no SAM (figures 6A,B).

Six weeks after implantation of permanent pacing system, the resting left ventricular outflow tract gradient has decreased to 8.8 mm Hg.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A,B) After dual-chamber pacing with a short atrioventricular delay, M-mode Doppler shows complete resolution of systolic anterior motion of the mitral valve and colour Doppler shows only mild mitral regurgitation.
Discussion
Acute heart failure caused by hypertrophic cardiomyopathy (HCM) is rare. Angina, palpitations, exertional dyspnoea, dizzy spells or syncope are common presenting symptoms of HCM.2 Our patient presented with the commonest clinically recognised phenotype of HCM affecting the anteroseptal region of the left ventricle.3 Acute ‘unmasking’ of HCM secondary to AV block is rare.4 Alteration in the normal AV coupling by AV block can induce significant LVOT obstruction in patients with HCM.5 6 HCM variants that have conducting system disease or accessory pathways as part of their phenotypic expression are recognised.7 His–Purkinje conduction abnormalities occur in approximately one-third of patients with HCM.8
Standard baseline medical treatment for HCM with LVOT obstruction includes β blockers, calcium channel antagonists and disopyramide.9 Patients with refractory symptoms may be considered for dual-chamber pacing with a short AV delay as a second-line option. Cardiac anatomy, age of patient and associated co-morbidities and local expertise will determine whether referral for surgical myectomy or alcohol septal ablation is more appropriate than a pacing strategy.10 Non-randomised studies in the 1990s suggested that dual-chamber pacing reduced the severity of LVOT obstruction and improved symptoms, but randomised controlled trials showed an equivocal correlation between the effects of pacing on the LVOT gradient and improvement in symptoms, quality of life and exertional capacity.9 11,–,13 The randomised trials have a number of limitations and longer term data have shown that dual-chamber pacing improves quality of life.14,–,16 In patients with refractory symptoms, surgical myectomy is superior to dual-chamber pacing in terms of reducing outflow tract gradient, improving symptoms and increasing exertional capacity.17
Dual-chamber pacing induces dyssynchronous interventricular contraction, altering the relationships between mitral valve structures and the interventricular septum during systole; thus, reducing LVOT obstruction.10 Pacing also reduces the severity of mitral regurgitation.18 In our patient, temporary RV apical pacing markedly reduced the LVOT gradient and severity of mitral regurgitation, which was primarily caused by acute AV block. Permanent dual-chamber pacing with short AV delay markedly reduced the LVOT gradient at rest and during exercise plus the severity of mitral regurgitation.
Heart failure is a complex medical condition with a poor prognosis when the problem cannot be found and corrected. A low threshold for cardiology referral and investigation may identify unusual causes of acute heart failure and improve outcomes.
Learning points
▶ Always evaluate patients with acute dyspnoea with an open mind.
▶ Patients presenting with acute heart failure should have echocardiography performed early in their management.
▶ Refer early for cardiology input if the initial response to medical management of heart failure is poor. Patients usually respond favourably within a few hours of standard treatment.
References
Footnotes
-
Competing interests None.
-
Patient consent Obtained.