Article Text

Statistics from Altmetric.com
Description
Rupture of mitral-aortic intervalvular fibrosa aneurysm is a rare complication of aortic valve endocarditis.1 A 43-year-old man presented with persistent fever and progressive dyspnoea of 3 months duration. On admission, he was in florid pulmonary oedema and clinical examination showed findings of severe aortic regurgitation. His electrocardiogram revealed complete heart block with junctional escape rhythm. The echocardiogram showed an aneurysm of mitral-aortic intervalvular fibrosa in parasternal long-axis view (figure 1 and video 1). Such aneurysms are recognised echocardiographically as an echo-lucent space in the mitral-aortic intervalvular fibrosa in the parasternal long-axis and short-axis views. The non-coronary cusp of the aortic valve was flail and colour Doppler echocardiography demonstrated rupture of the aneurysm with communication to both left ventricular outflow tract and left atrium. There was severe aortic regurgitation with mild mitral regurgitation. The short axis view revealed large vegetation attached to the non-coronary cusp of aortic valve with root abscess formation (figure 2 and video 2). He died due to refractory heart failure. This case illustrates possible complications of aortic valve endocarditis flail leaflet, severe aortic regurgitation, rupture of intervalvar fibrosa aneurysm, root abscess and complete heart block.

Parasternal long-axis view demonstrating the aneurysm in the mitral-aortic intervalvular fibrosa (*). Colour Doppler across left ventricular outflow tract (LVOT) reveals pulsatile nature of the aneurysm with communication to both LVOT and left atrium. The flail non-coronary cusp (indicated by arrow) with severe aortic regurgitation can also be seen.

{kind=link}
{kind=link}
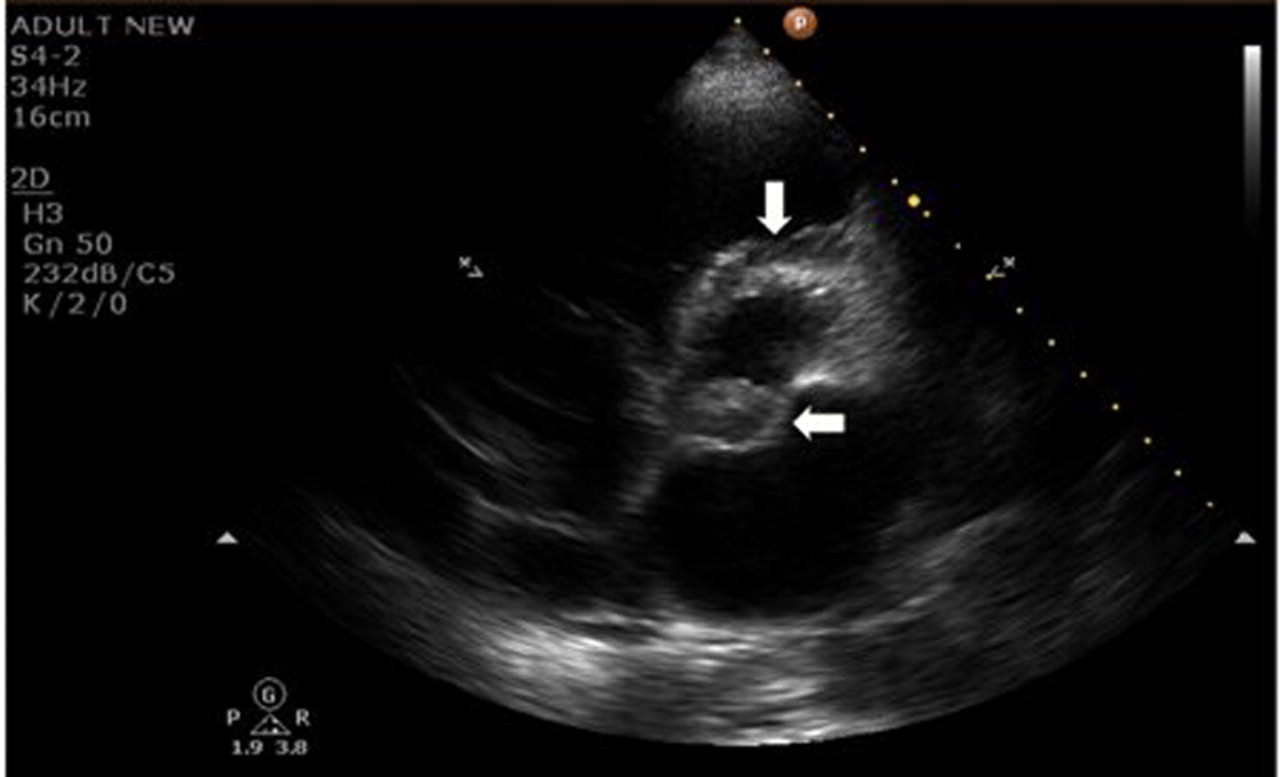
Parasternal short-axis view showing large vegetation (horizontal arrow) attached to the non-coronary cusp of the aortic valve with root abscess in the 12’ o clock position (vertical arrow).
Parasternal long-axis view demonstrating the aneurysm in the mitral-aortic intervalvular fibrosa. Colour Doppler across LVOT reveals pulsatile nature of the aneurysm with communication to both LVOT and left atrium. The severe aortic regurgitation can also be seen with flail aortic valve cusp.
Parasternal short-axis view showing large vegetation attached to the non-coronary cusp of the aortic valve with root abscess in the 12’ o clock position.
References
Footnotes
-
Competing interests None.
-
Patient consent Obtained.