Article Text

Statistics from Altmetric.com
Description
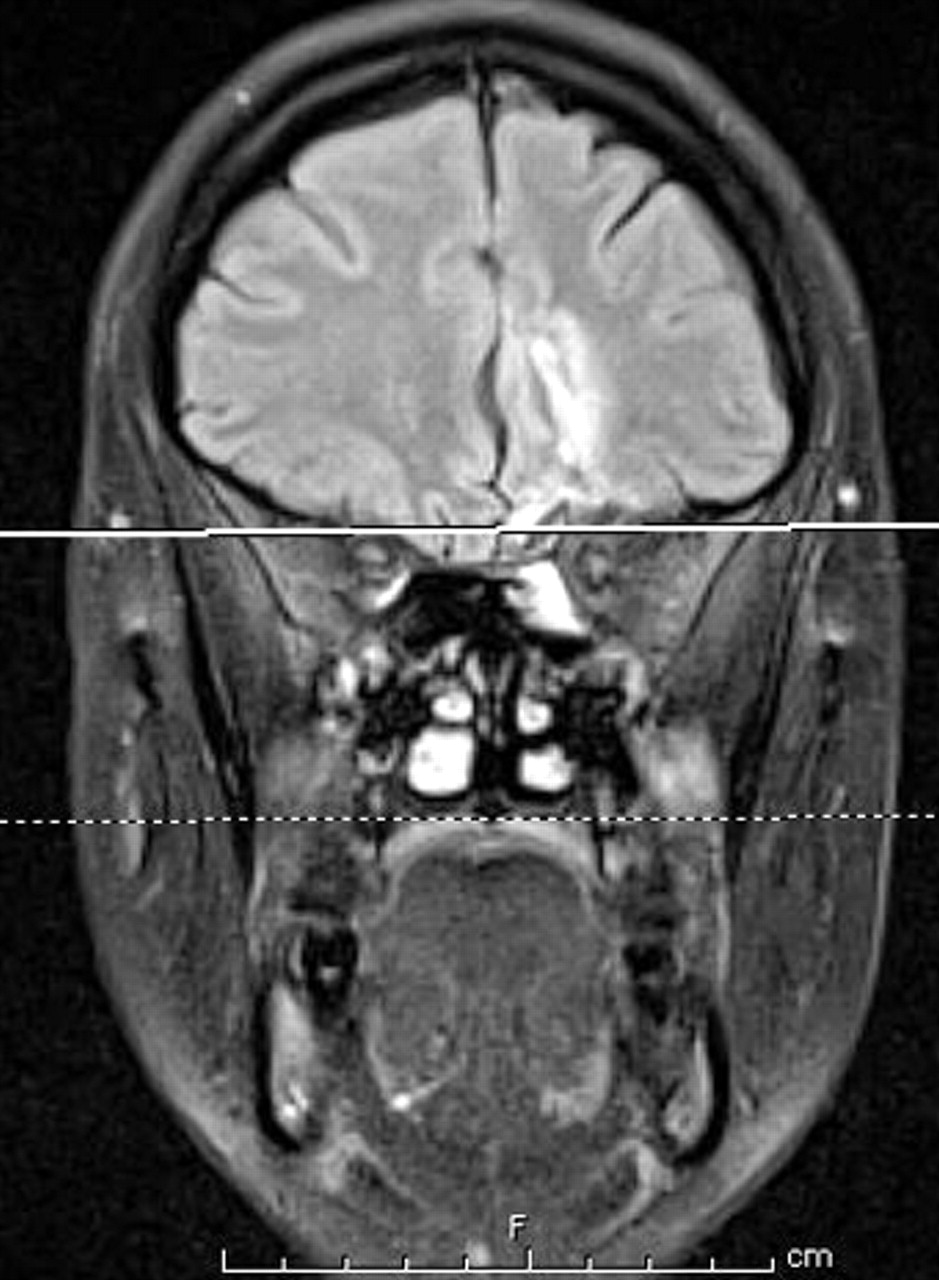
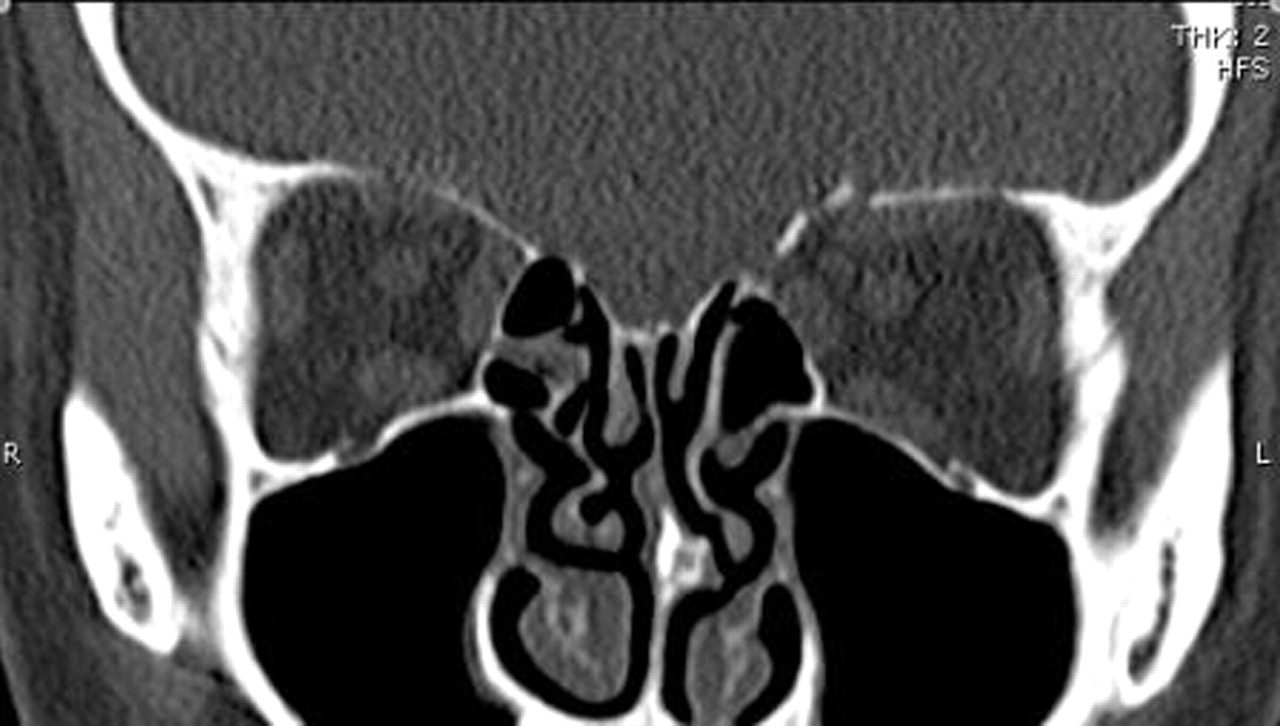
A 43-year-old woman presented to accident and emergency after being assaulted. During the incident she was stamped on the head with a stiletto. On examination, she was described as being ‘intoxicated’ but denied drinking or illicit drug use. However, her Glasgow coma score remained fifteen throughout. A small, left upper lid laceration was noted and sutured. No other injuries were detected and consequently she was discharged. One month later she re-presented with diplopia and headaches. She also complained of mild expressive dysphasia and irritability. Examination of her ocular motility revealed a pattern consistent with an acquired Brown’s syndrome. CT and MRI were requested (figures 1 and 2) which showed a comminuted fracture of the left medial orbital roof and a cerebral laceration of the left frontal lobe extending to the anterior horn of the lateral ventricle. No form of radiological imaging was requested at presentation. Consequently, a serious intracranial injury was missed. Plain orbital x-rays may have demonstrated the fracture and CT/MRI of the orbits and brain would have conclusively revealed an abnormality. Had the true extent of the patient’s injuries been known, her management would have changed considerably. At a minimum she would not have been discharged, she would have been treated with broad spectrum antibiotics and a neurosurgical opinion would have been sought. Retrospectively, this event was clearly a ‘near miss’. Apparently, innocuous wounds may conceal serious injuries that can easily be missed if radiological imaging is not performed following peri-ocular injuries sustained by sharp objects.
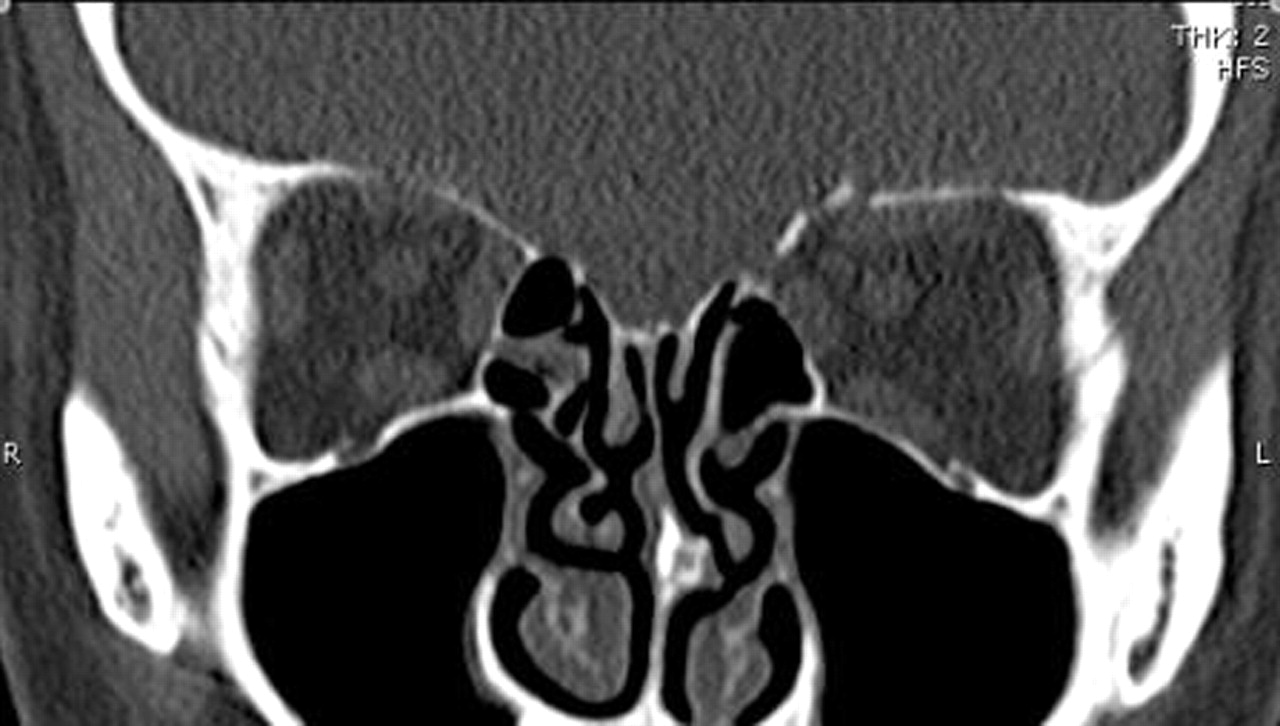
CT showing comminuted fracture of the left, medial orbital roof.
{kind=link}
{kind=link}
MRI demonstrating a cerebral laceration of the left frontal lobe with associated gliosis and old parenchymal haemorrhage.
Footnotes
-
Competing interests None
-
Patient consent Obtained