Article Text

Statistics from Altmetric.com
Description
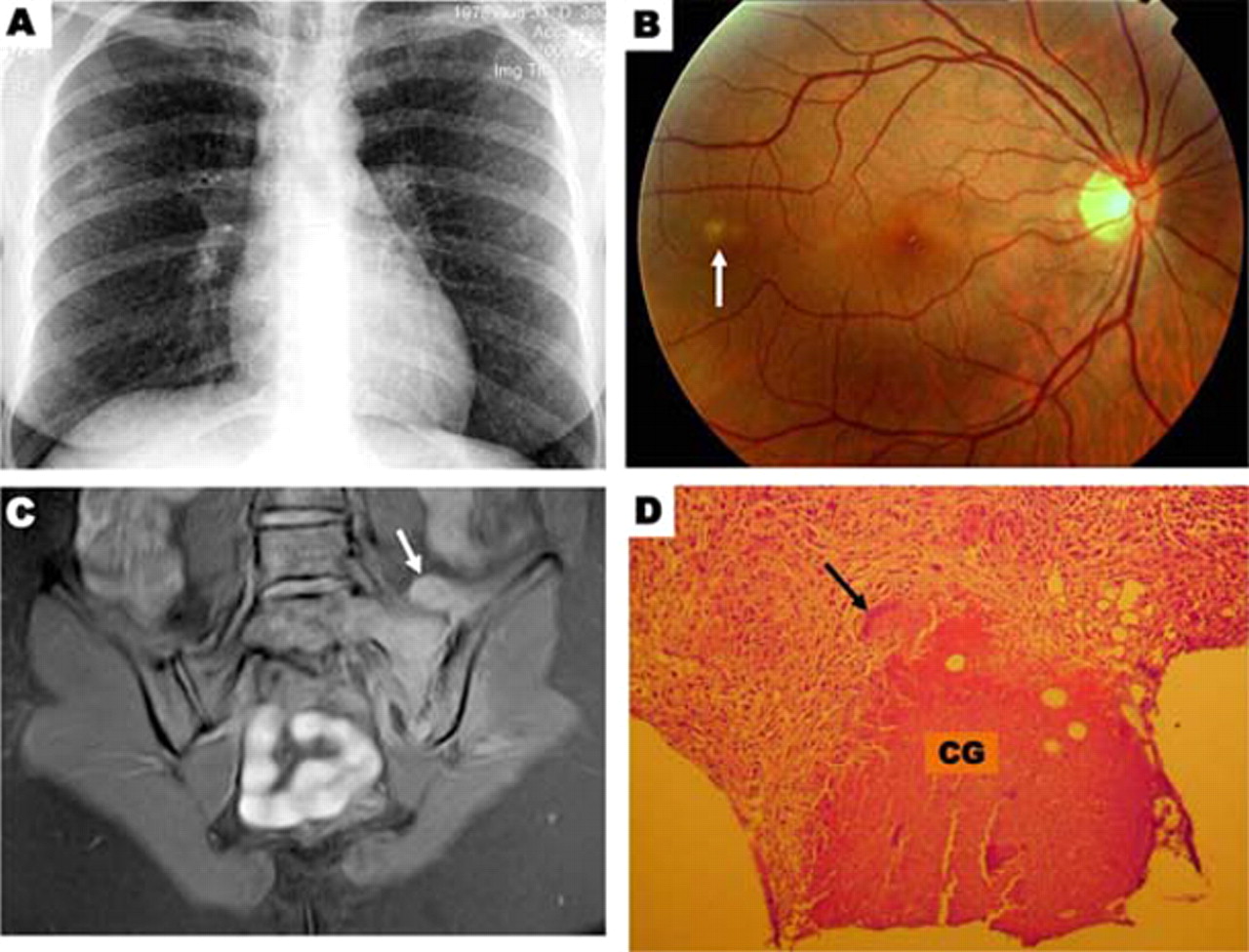
A previously healthy 31-year-old woman presented to our emergency department with a 1-month history of fever, non-productive cough, malaise and weight loss. She also reported having had low back and left buttock pain for the last 5 months. Stress tests of the sacroiliac joint, namely the lateral pelvic compression test, the flexion, abduction and external rotation of the hip joint test and the Gaenslen’s test (hyperextension of the hip with pelvis fixed by flexion of opposite hip and knee) were positive, that is, they elicited pain on the left sacroiliac joint. Chest radiography performed on admission showed multiple, faint small nodules in both lungs (figure 1A). A subsequent fundus examination revealed a greyish-white oblong patch with indistinct edges in the right eye (figure 1B), which was ascribed to choroidal tubercle by an ophthalmologist. MRI showed signs of left sacroiliitis with accompanying iliopsoas abscess (figure 1C). The histopathological analysis of the bone marrow biopsy samples from the right iliac crest revealed multiple caseating granulomas with Langhan’s-type giant cells (figure 1D). Tuberculin skin test and serology for the human immunodeficiency virus were negative. Specimens from bronchioalveolar lavage fluid, transbronchial biopsy, urine, blood and bone marrow biopsy were negative for acid-fast bacilli as well as for Mycobacterium tuberculosis culture and PCR testing. Considering that there was no evidence for other alternative aetiology, disseminated tuberculosis was diagnosed on the basis of miliary chest pattern, choroidal lesion and pathological findings. The patient was treated with antituberculous drugs for 9 months. She had a full clinical and radiological recovery.
{kind=link}
Chest x-ray, revealing a micronodular pattern in both lungs (A). Ophtalmological examination, showing a choroidal tubercle in the left eye (B; arrow). MRI, revealing left sided contrast enhancement in the sacroiliac space and iliac and sacral bones as well as iliopsoas abscess (C; arrow points out to the abscess). Finally, pathological findings in a bone biopsy specimen (D; CG, caseating granuloma; arrow indicates a Langhan’s-type giant cell; hematoxylin-eosin stain).
Disseminated tuberculosis is uncommon, especially in immunocompetent patients.1 The broad spectrum of its possible presentations makes diagnosis difficult unless clinical suspicion of disease is high. It is well known that, sometimes, current diagnostic tests can not reveal the presence of M tuberculosis.2 Since early initiation of treatment is essential to achieve a favourable outcome, clinicians should keep in mind that ophthalmoscopic examination3 and histopathologic study2 may be important to reach a timely diagnosis of the disease.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.