Article Text

Statistics from Altmetric.com
Description
A 60-year-old woman was admitted to our emergency department with respiratory distress. Her thorax had undergone gradual deformation over the past 3 years during which time she had refused to seek medical intervention. Her ADL (activities of daily living) had been full and she had worked as a dancing instructor before her thorax began to change shape. On admission, she was alert, but had severe dyspnoea with low arterial oxygen saturation. Chest x-ray, CT (figure 1) and three-dimensional CT reconstruction images (figure 2) revealed severe thoracic deformity. Serum biochemistry showed increased serum levels of alkaline phosphatase (1289 IU/l; normal 115–359 IU/l), intact parathyroid hormone (858 pg/ml; normal 10–65 pg/ml) and brain natriuretic peptide (1481 pg/ml; normal 0–18 pg/ml) in addition to low levels of calcium (7.9 mg/dl; normal 8.7–10.3 mg/dl), 1.25-(OH) 2 Vit D (7.0 pg/ml; normal 20–60 pg/ml) and 25-(OH) Vit D (<5 ng/ml; normal 7–41 ng/ml). Bone mineral density, expressed as T-score, was decreased significantly (lumbar spine (L2–L4) - 6.8; total hip - 7.31). The patient was diagnosed with osteomalacia associated with respiratory and cardiac failure. She remained unresponsive to alfacalcidol treatment and non-invasive positive-pressure ventilation and died 1 month after admission. As this patient’s history included anorexia nervosa in later childhood and ovarian resection 12 years ago, we consider she had osteoporosis before development of the thoracic deformation. Various factors may cause vitamin D insufficiency and osteomalacia. These include a lack of vitamin D intake or absorption, lack of ultraviolet (UV) irradiation, drug-induced or oncogenic changes, chronic renal failure and acidosis.1 2 She followed a strict vegetarian diet and was conscious of UV protection. In addition, due to an injury of the urinary duct during an ovarian operation her right kidney had lost function, and owing to lowering of ADL she had an inclination to stay indoors. These factors appeared to have contributed to the onset of osteomalacia and severe thoracic deformity. Previous reports have described osteomalacia with thoracic deformity,3 although the current case is rare as it was associated with severe respiratory insufficiency, caused by various different factors complicated by osteoporosis.

Chest x-ray (A) and CT (B) revealed severe thoracic deformity.
{kind=link}
{kind=link}
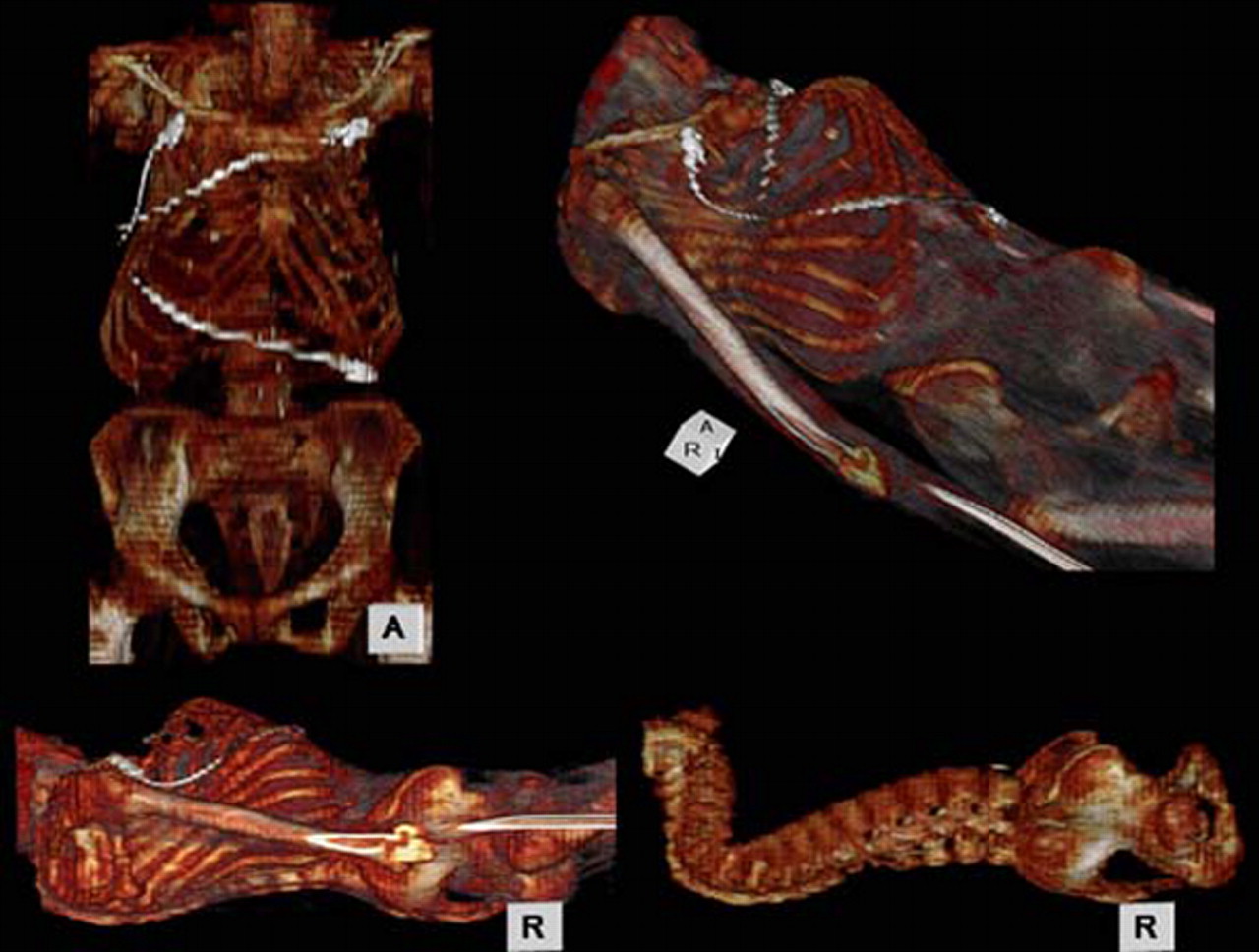
Three-dimensional CT reconstruction images showed costal protrusion and striking posterior curvature of the thoracic spine.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.