Article Text

Statistics from Altmetric.com
Description
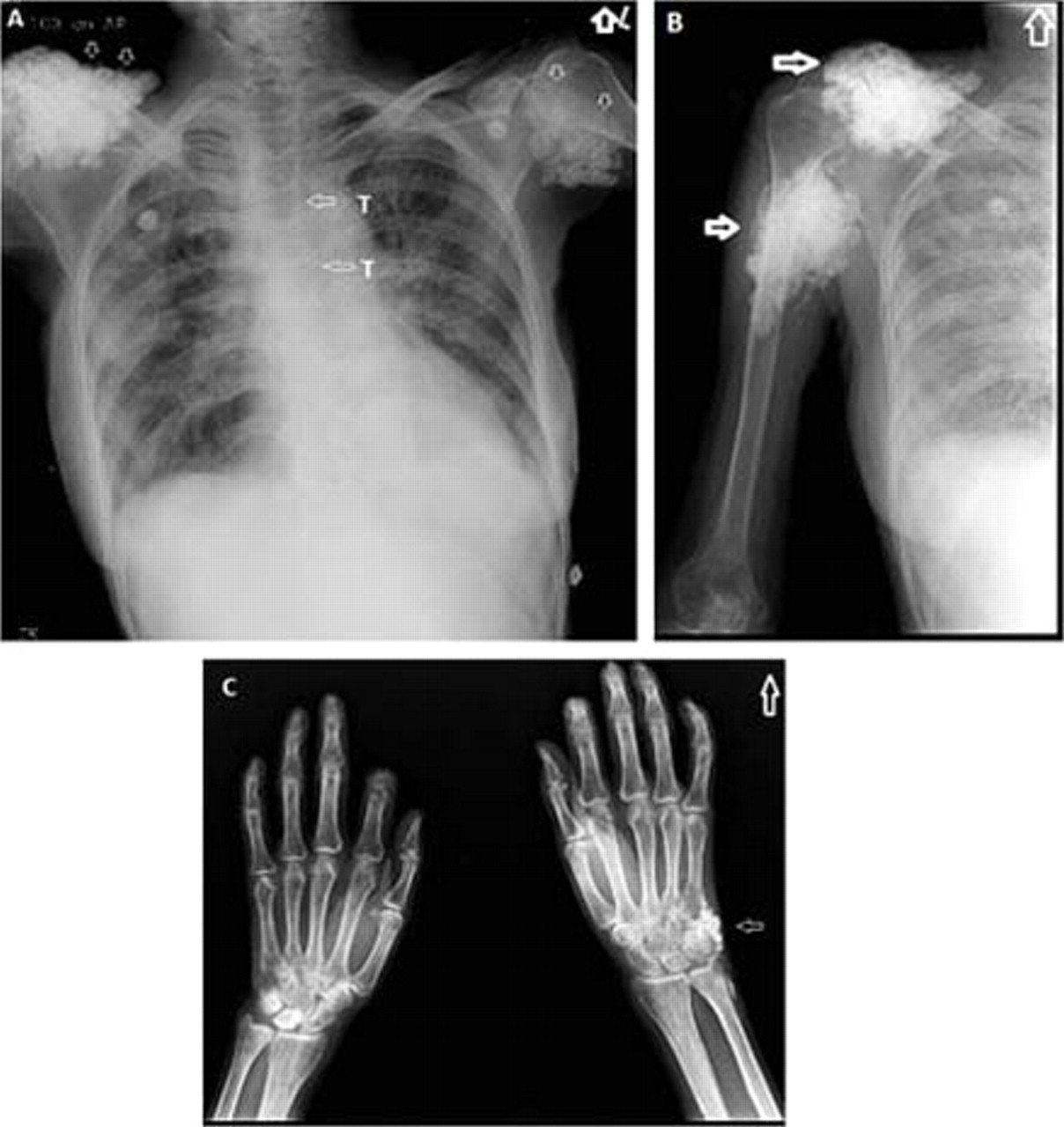
A 74-year-old lady was admitted with complaints of breathlessness of 1-week duration. She had been diagnosed as limited scleroderma, 10 years back; however, she was not on any medications. Chest radiograph was suggestive of alveolar oedema; extensive calcification of soft tissue around the shoulder joints was noted bilaterally (figure 1A, arrows). Additional radiographs revealed calcification around the right shoulder joint (figure 1B, arrows) and wrist (figure 1C, arrow). The patient had no symptoms related to the same. She had critical stenosis in her left anterior descending artery for which she underwent an angioplasty and stent placement. Calcinosis cutis (Cc) is the deposition of insoluble calcium salts (hydroxyapatite crystals and amorphous calcium phosphates) in the skin.1 2 First described by Virchow in 18553; it is classified into four major types according to aetiology as dystrophic, metastatic, iatrogenic and idiopathic.
{kind=link}
(A) Chest radiograph showing calcification of soft tissue around the shoulder joints bilaterally (arrows). T denotes tracheal calcification. (B) Radiograph of right shoulder joint showing soft tissue calcification (arrows). (C) Radiograph of wrist joints showing calcification (arrow).
Metastatic calcification arises in the setting of abnormal calcium or phosphate metabolism and is generally associated with hypercalcaemia and/or hyperphosphataemia. Examples include hyperparathyroidism, paraneoplastic hypercalcaemia and chronic renal failure. Idiopathic Cc occurs in the absence of known tissue injury or systemic metabolic defect. Examples include idiopathic Cc of scrotum, penis or vulva, Milia-like idiopathic Cc4 and transplant-associated idiopathic Cc.5 Iatrogenic Cc arises secondary to parenteral administration of calcium or phosphate,6 repeated heel sticks in the newborn, prolonged use of calcium-containing electrode paste in diagnostic procedures such as electroencephalography.
In connective tissue diseases, calcinosis is mostly of the dystrophic type and it seems to be a localised process rather than an imbalance of calcium homeostasis. Serum calcium, phosphorus and alkaline phosphatase levels are typically normal. Calcium deposits may be intracutaneous, subcutaneous, fascial or intramuscular.
Complications of Cc include pain, cosmetic disfigurement, persistent ulceration with infection and mechanical compromise.
Work-up for Cc includes serum calcium, inorganic phosphate, alkaline phosphatase and albumin. Imaging studies include radiographs, CT and bone scintigraphy. On biopsy, granules and deposits of calcium are seen in the dermis on Von Kossa and alizarin red stains.
The pharmacological treatment is difficult and a variety of drugs including bisphosphonates, intralesional corticosteroids, warfarin and diltiazem have been tried with limited success. The local excision of painful or ulcerated nodule is an option but local recurrence is common.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.