Article Text

Summary
A man in his late 20s presented with a painless swelling in his left axilla accompanied with nocturnal sweating. On examination, there was a well circumscribed, pulsatile lump within the axilla. Subsequent imaging revealed an axillary artery aneurysm with thrombus within. Subsequent surgical repair was undertaken. Subsequent histological examination of the vessel revealed features characteristic of angiolymphoid hyperplasia with eosinophilia.
Statistics from Altmetric.com
Background
This is a rare cause of an axillary artery aneurysm in a young patient and brings together dermatology, rheumatology and vascular surgery.
Case presentation
A man in his late 20s presented with a painless swelling in his left axilla. He also had a long history of nocturnal sweating with no history of weight loss or fatigue. On examination, there was a large, well circumscribed lump measuring 3 × 2.5 cm within the apex of the left axilla. The mass was pulsatile, firm and non-tender. General examination was otherwise unremarkable; in particular, there were neither skin lesions nor palpable lymphadenopathy.
Investigations
Biochemical and haematological investigations were normal apart from a mildly raised eosinophil count of 0.5 × 109/l (upper limit of normal 0.4 × 109/l).
Doppler ultrasound confirmed a 2.9 cm long × 1.8 cm wide aneurysm of the distal axillary artery with evidence of an irregular thrombus present within.
Differential diagnosis
Angiolymphoid hyperplasia with eosinophilia (ALHE) has been known by a variety of different names, such as epithelioid haemangioma, pseudopyogenic granuloma, inflammatory angiomatous nodule, papular angioplasia, subcutaneous angioblastic lymphoid hyperplasia with eosinophilia and lymphofolliculosis, intravenous atypical vascular proliferation and histiocytoid haemangioma.1 This extensive list of nomenclature reflects the spectral variation in microscopic presentations of ALHE encountered by past investigators and, not least, the divided opinion as to whether the pathogenesis of the lesion is truly neoplastic or a reactive phenomenon.
There has been controversy over the exact relationship between Kimura’s disease (KD) and ALHE, where the two terms have been used interchangeably in many articles. KD was first described by Chinese authors Kimm and Szeto2 in 1937 and later made widely recognised by Kimura in 1947. KD is a chronic inflammatory disease of unknown aetiology usually presenting as solitary or multiple subcutaneous nodules in the head and neck region, often involving the parotid or submandibular salivary glands. KD is associated with regional lymphadenopathy; this may become generalised in longstanding disease,3 and systemic eosinophilia with raised IgE levels. It is most prevalent in Asians with 85% of cases occurring in males.
Although KD has been thought to be integral to the spectrum of ALHE in the past, histological features show that these conditions represent two separate disease entities.4 KD is characterised by lymphoid nodules with germinal centres which may extend from the dermis to the underlying fascia and muscles. Lesions show a distinct eosinophilic infiltrate with microabscesses. Vascular proliferation is not always present; however, when seen, there are many canalised capillaries lined by flat endothelial cells. Systemic eosinophilia is almost always present, seen in approximately 98% of cases in comparison to 20% in ALHE.5
In contrast to KD, ALHE lesions are superficial containing blood vessels of varying luminal sizes, some of which may not be canalised, lined by distinctive endothelium of an epithelioid appearance. Eosinophilic abscesses are not seen and peripheral eosinophilia is not always present. KD is thought to be an allergic response, owing to the presence of eosinophilia and elevated IgE levels, whereas ALHE is believed to be a true neoplasm of the endothelium.6
ALHE has previously been reported three times arising from the radial artery. It has not, however, been reported as arising from the axillary artery. In this case, there was no association with local trauma or infection. While ALHE is a rare condition it should be considered in the presence of peripheral vessel aneurysm formation, especially in the presence of skin lesions.
Treatment
Subsequent surgical repair of the axillary artery aneurysm involved complete excision of the defect followed by end-to-end interposition of cephalic vein graft, taken from the patients left arm.
Outcome and follow-up
Histological examination of the excised segment revealed destruction of the arterial wall with a heavy chronic inflammatory infiltrate (including lymphocytes, plasma cells, macrophages and eosinophils) with prominent endothelial cells of epithelioid morphology. These features are characteristic of ALHE.
The graft remains patent with normal limb function at 1 year.
Discussion
ALHE is characterised by solitary or multiple subcutaneous nodules with a predilection for the head and neck region. It presents in patients between 20 and 50 years of age, with a mean age at onset of 30–33 years.7 The incidence of ALHE is greater in females than in males.8 The condition is more commonly encountered in the Asian population followed by Caucasians, it is rare in the black population.
The subcutaneous lesions associated with ALHE may vary in colour, shape and size. Ranging from red to brown in colour, the lesions may be smooth or centrally eroded with crusting. The size of a single lesion may vary from 0.2 to 8 cm, most commonly measuring 0.5–2 cm. Approximately 80% of patients demonstrate solitary lesions, while 20% have multiple lesions clustered in one area.1 They are most commonly seen in the peri-auricular area, forehead or scalp. Rare sites of involvement include the shoulders, hands, breasts and penis.7 ALHE tends to affect the skin and subcutaneous tissues, however, it has also been described in other tissues, such as the orbit, oral mucosa, liver, spleen, heart, bone and blood vessels.9 Systemic eosinophilia of 6–34% is seen in 20% of patients.1 Regional lymphadenopathy and arteriovenous shunts have occasionally been reported but are inconsistent features.
Lesions may be asymptomatic, painful on palpation or pruritic. Some patients experience tumour pulsation and bleeding, either spontaneously or after minor frictional trauma.
The pathophysiology of this benign condition is unclear. A history of local trauma or infection is found in 9% of patients. The period between trauma and discovery of a lesion ranges between 7 months and 20 years, with a median interval of 30 months.1
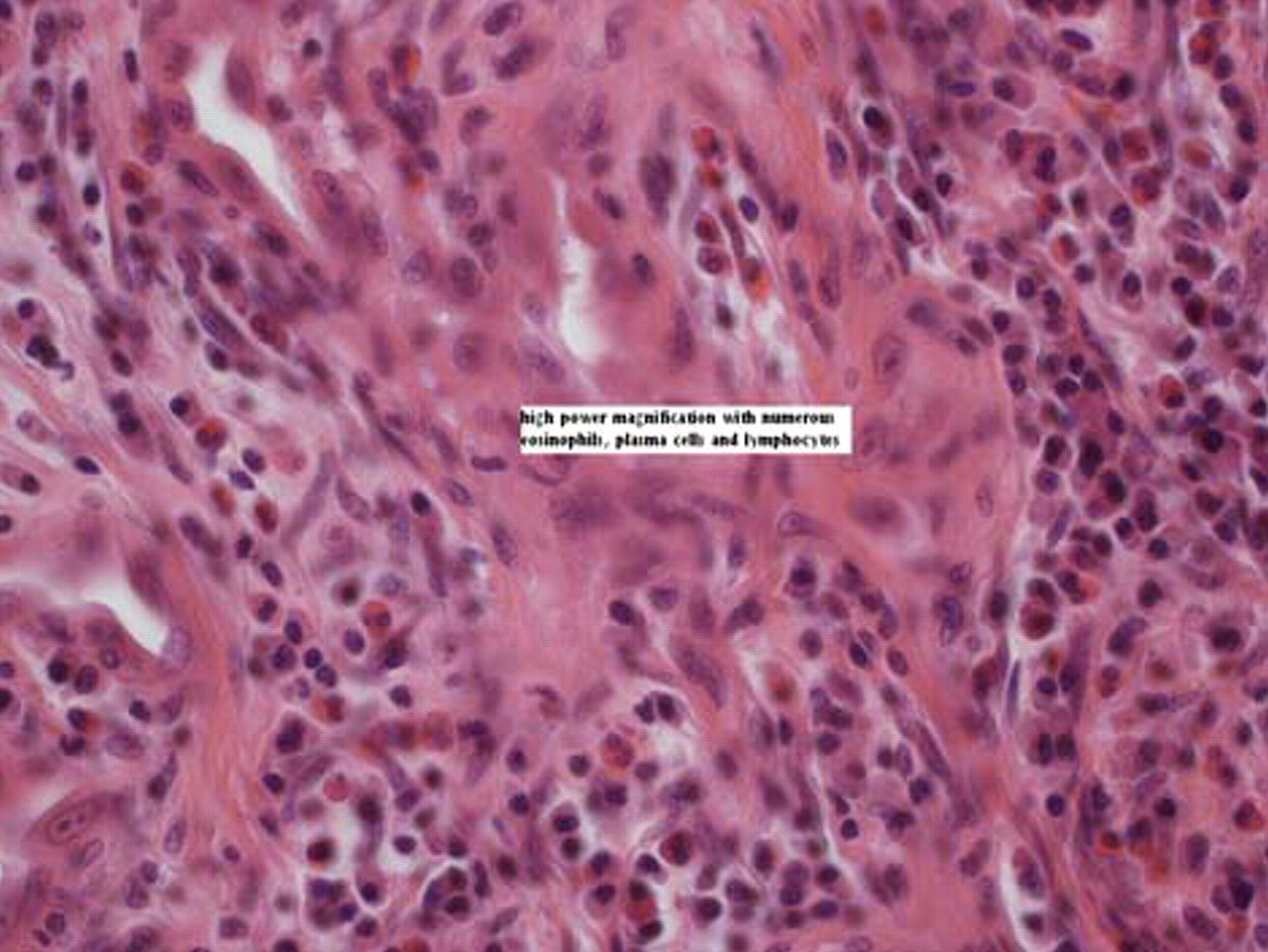
The histology of ALHE shows a distinct proliferation of blood vessels with thickened walls (figure 1). These are lined with prominent epithelioid endothelial cells said to have a cobblestone appearance, some of which contain cytoplasmic vacuoles.10 Additionally, a characteristic chronic inflammatory infiltrate is seen in the perivascular and interstitial tissue, comprised of lymphocytes, plasma cells and eosinophils (figure 2). Eosinophils usually account for 5–15% of the infiltrate, though in rare cases eosinophils may account for up to 50%.7 Aggregation of lymphocytes is typical with a tendency to form lymphoid follicles. The lack of sinus structure indicates that these follicles arise in the subcutaneous tissue.11

AHLE demonstrating distorted brachial artery and classical small vessel proliferation.

{kind=link}
{kind=link}
Higher power magnification demonstrating dense inflammatory infiltrate.
Two types of ALHE lesion are described by Wells and Whimster. The early lesion demonstrates a predominance of rapidly proliferating atypical vasculature. However, late lesions illustrate maturation of these atypical blood vessels with thickened walls along with a high prevalence of lymphoid follicles seen towards the periphery of the lesion.12
ALHE rarely regresses spontaneously; however, malignant transformation does not occur. Several treatment modalities have been used, including intralesional corticosterioid injections, interferon α2b, cytotoxic agents, cryotherapy, electrodessication, pulse-dye laser and carbon dioxide laser. Surgical excisions that include the arterial and venous segments at the base of the lesion are most successful, with no reported recurrence after 1 year of follow-up.13
Learning points
▶ Consider vasculitis as a cause of peripheral artery aneurysm.
▶ Complications of vasculitis induced aneurysms are the same as more common traumatic and atherosclerotic aneurysms.
▶ Surgical treatment of the aneurysm is required.
Footnotes
-
Competing interests None.
-
Patient consent Not obtained.