Article Text

Statistics from Altmetric.com
Description
A 28-year-old woman presented with recurrent syncope, usually precipitated by anxiety.
On examination, she had a low blood pressure of 112/72 mm Hg with normal heart sounds and showed no features suggestive of genetic abnormalities. ECG, Holter and treadmill stress tests were normal. Transthoracic (figure 1) and transoesophageal (figure 2) echocardiography demonstrated non-obstructive cor triatriatum. A diagnosis of vasovagal syncope with incidental cor triatriatum was made.

Transthoracic apical four chamber view showing a horizontal structure crossing the left atrial chamber (white vertical arrow). The mitral valve is at the level of the white horizontal arrow. LV, left ventricle; RA, right atrium.

{kind=link}
{kind=link}
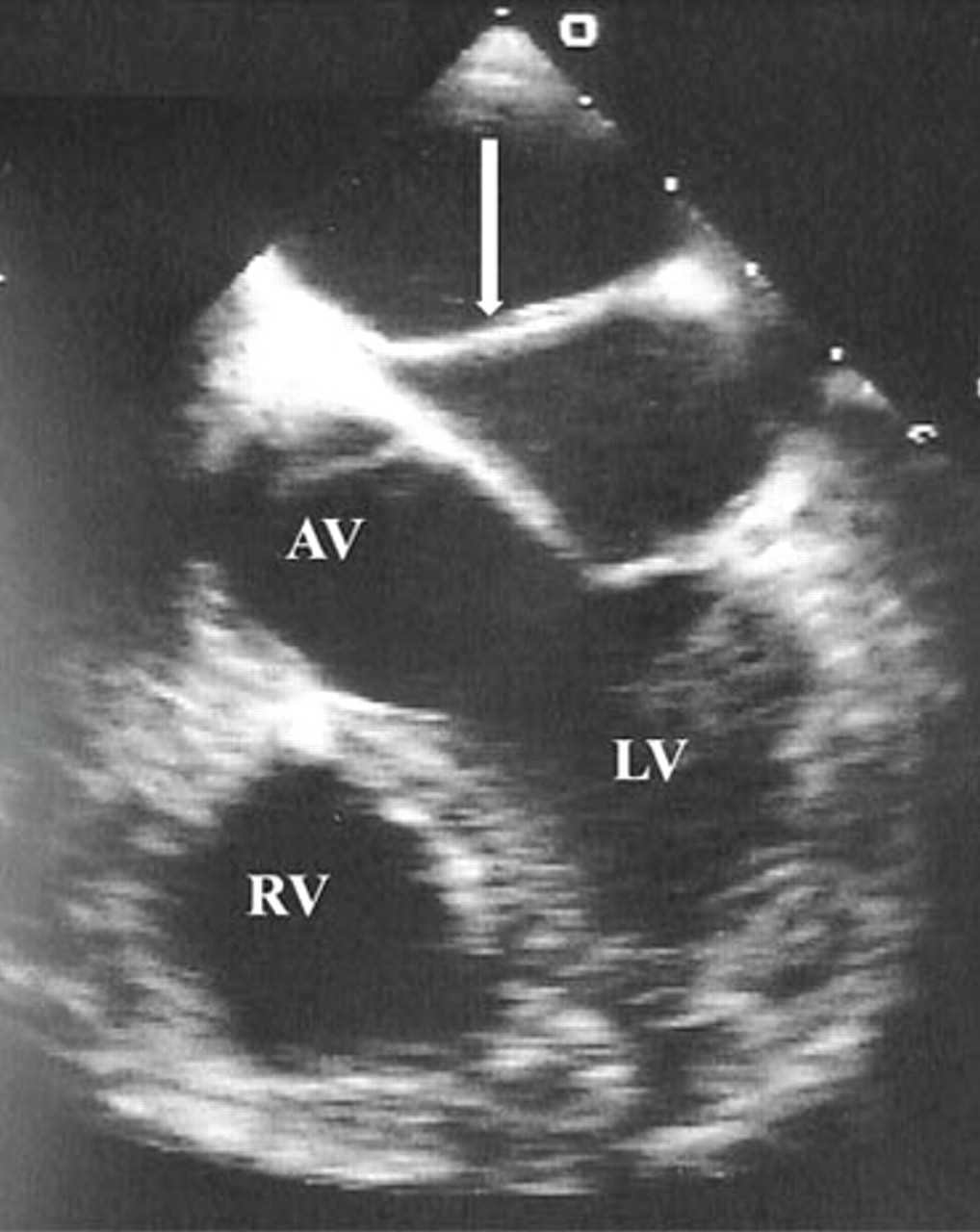
Transoesophageal view showing a structure crossing the chamber of the left atrium (broad white arrow). AV, aortic valve; LV, left ventricle; RV, right ventricle.
Cor triatriatum consists of a fibromuscular membrane dividing the left atrium into a posterosuperior chamber receiving blood from the pulmonary veins and an anteroinferior chamber containing the left-atrial appendage and mitral orifice. It represents 0.4% of congenital cardiac anomalies,1 and is associated with other cardiac defects in 70–80% of cases,2 anomalous pulmonary venous drainage being the most common. Echocardiography is crucial to determine the transmembrane gradient, pulmonary vein drainage and associated defects.1
The natural history of cor triatriatum depends on the size of communication between chambers and presence of associated abnormalities. When small, it usually presents in infancy with reduced cardiac output, pulmonary venous hypertension and cardiac failure. Untreated, mortality approaches in 75% of the patients. Larger orifices may present incidentally, as described, or in young adulthood with features similar to mitral stenosis. Surgical excision of the membrane is the definitive treatment.
If present, a patent foramen ovale (PFO) or atrial septal defect permits decompression of the proximal chamber into the right atrium, with a significantly improved prognosis. Presentation in adulthood is unusual but late conversion to a symptomatic state may be caused by fibrosis and calcification around the orifice, the development of mitral regurgitation or atrial fibrillation.
Our patient was asymptomatic from her PFO. We have not recommended routine antibiotic prophylaxis but the patient was counselled to be cautious with infection, dehydration, pregnancy or surgical interventions. We anticipate annual cardiac surveillance.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.