Article Text

Statistics from Altmetric.com
Description
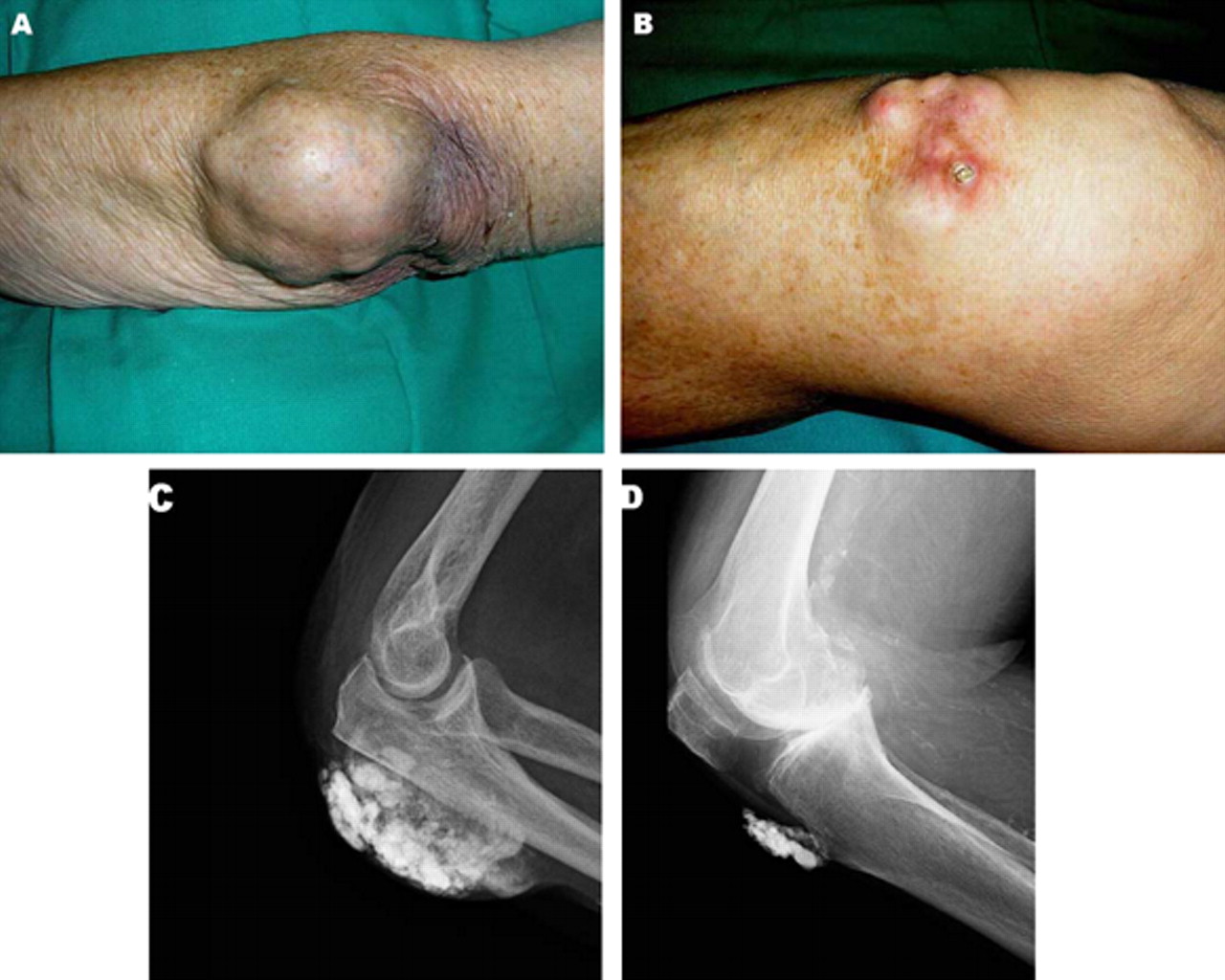
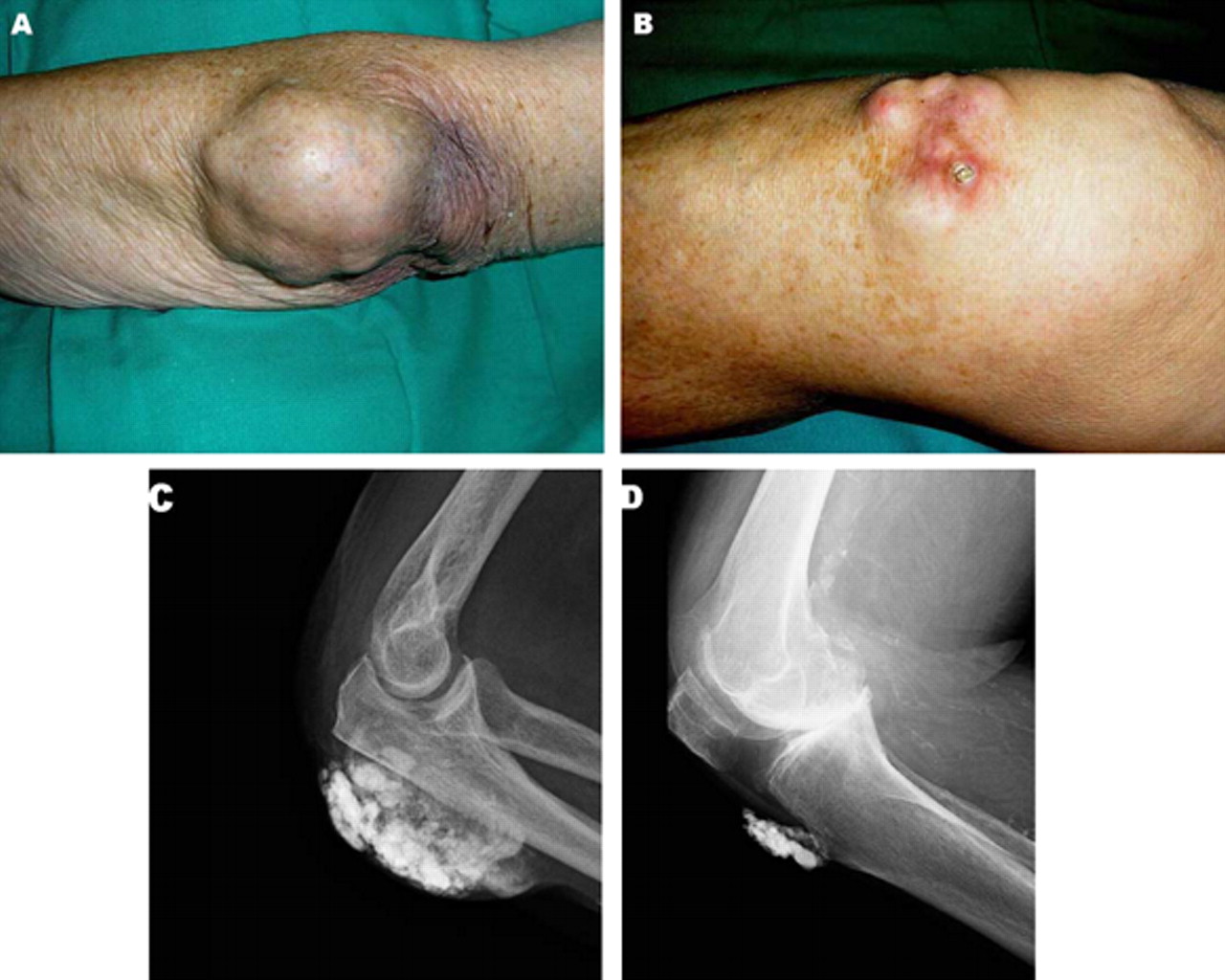
An 87-year-old woman with a history of hypertension, atrial fibrillation, and mixed connective tissue disease was admitted to hospital because of heart failure. Besides clinical signs of ventricular dysfunction, physical examination showed painless, subcutaneous nodules that had developed during the past 10 years on her left elbow (figure 1A) and knees (figure 1B, right knee; note a large deposit breaking through the skin). A radiograph of the left elbow (figure 1C) and right knee (figure 1D) demonstrated multiple, heterogeneous soft-tissue calcified masses suggestive of calcinosis cutis. Her serum level of calcium, phosphate, intact parathyroid hormone and rheumatoid factor as well as renal function parameters were within normal limits. She afterwards died due to hospital-acquired pneumonia.
{kind=link}
Appearance of the left elbow (A) and the right knee (B) on clinical examination. Left elbow (C) and right knee (D) radiograph.
Calcinosis cutis, described by Virchow1 in 1855, refers to the deposition of insoluble calcium salts into the skin and subcutaneous tissue. It has been divided into four groups: metastatic, iatrogenic, idiopathic and dystrophic.2 Metastatic calcification is related to abnormal calcium or phosphate metabolism and is generally associated with hypercalcaemia and/or hyperphosphatemia. Iatrogenic calcinosis cutis arises as complication of a therapeutic3 or diagnostic procedure. It has been associated with subcutaneous injection of calcium-containing heparins,3 extravasation of calcium gluconate and use of calcium-containing electrode compounds for electromyographic or electroencephalographic examination. Idiopathic calcinosis cutis occurs in the absence of known tissue injury or systemic metabolic defect. Finally, the dystrophic form is the most commonly described. Various conditions can cause this type of calcinosis, including connective tissue diseases, infection, other inflammatory processes, chronic venous stasis, cutaneous neoplasm, trauma and inherited disorders. The exact mechanism remains unclear although local inflammation may have a role in its pathogenesis.4 Treatment of calcinosis cutis in this setting have only marginal benefit, diltiazem and aluminum hydroxide antacids having been used.4 However, early, effective management of the underlying disorder could reduce the development of such abnormality. Given that there was no other predisposing condition for calcinosis besides mixed connective tissue disease, we believe our patient had dystrophic calcinosis related to such disorder. The lack of any of the other diagnostic criteria for rheumatoid arthritis and the fact that almost all rheumatoid nodule formers have positive tests for rheumatoid factor made the diagnosis of rheumatoid nodules very unlikely. In addition, these nodules usually appear as non-calcified subcutaneous masses.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.