Article Text

Statistics from Altmetric.com
Description
An elderly farmer presented with a swelling over his left eye associated with headache and loss of vision of 1 week’s duration. Having taken steroids off and on for chronic dermatitis for the past 4–5 years, he was diagnosed with diabetes 4 months previously and was prescribed oral antidiabetic drugs. Unfortunately, he had stopped taking his medications 15 days before presentation.
Examination of the patient’s left eye revealed (fig 1) periorbital swelling, complete ptosis, and ΙΙ, ΙΙΙ, ΙV, VΙ cranial nerve palsy (complete ophthalmoplegia) was present. Perception of light was absent and the pupil was dilated and fixed. His right eye was normal.

Complete ophthalmoplegia of left eye.
Nasal examination showed a blackish firm deposit with mucopus on the left side near the middle meatus. Clinical investigation revealed leucocytosis with predominant neutrophilia and high random blood sugars, and the patient was put on antibiotics and insulin therapy.
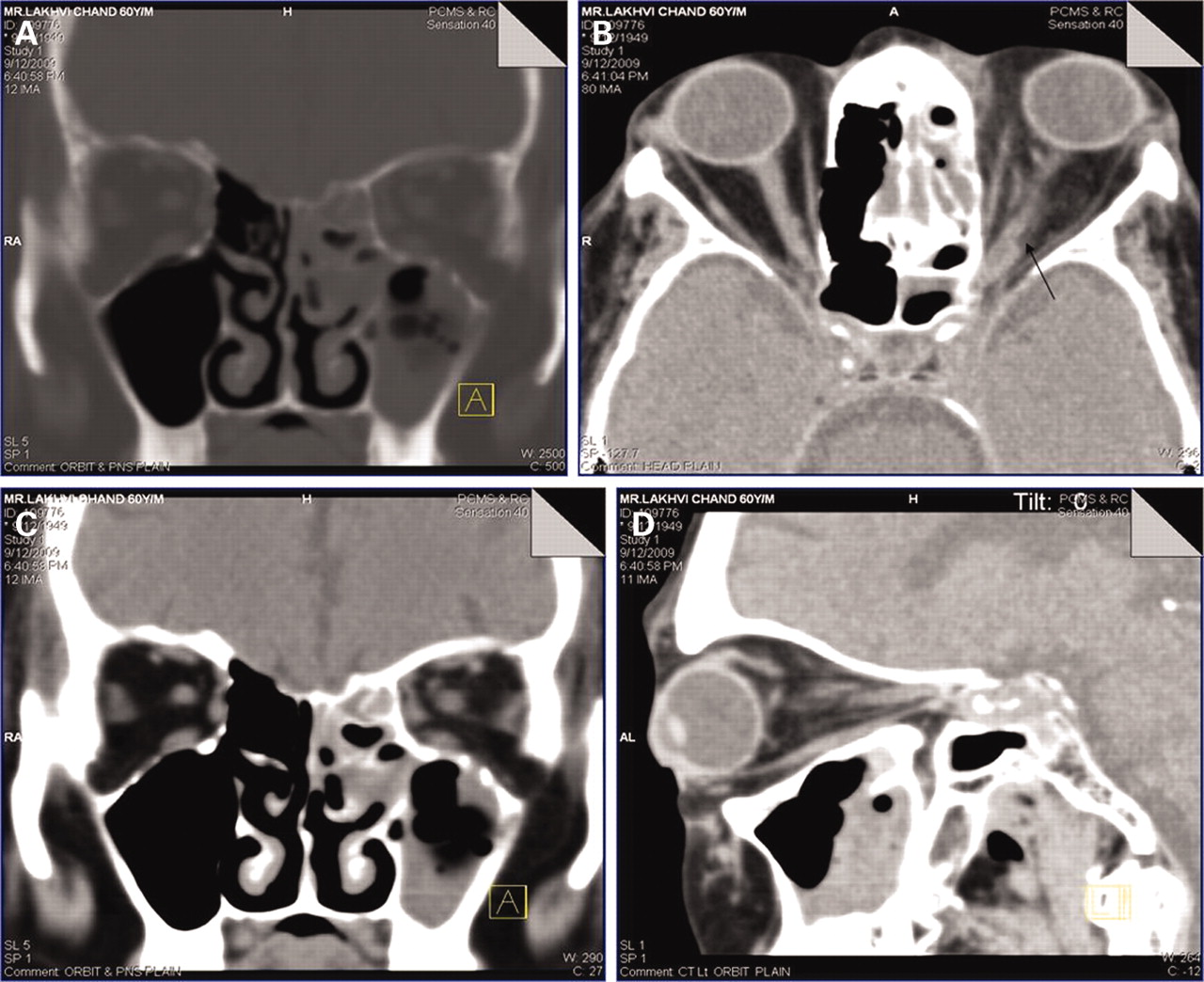
Plain coronal computed tomography (CT) scan of the paranasal sinuses and orbits was undertaken along with a potassium hydroxide (KOH) preparation of the nasal swab which showed significant findings (fig 2A–C and fig 3).

(A) Plain coronal computed tomography (CT) paranasal sinus (PNS) scan showing heterogeneous soft tissue density in the left maxillary sinus, and anterior and posterior ethmoid air cells. (B) Plain axial CT orbit showing increased thickness of optic nerve sheath complex with irregular margins, retro-orbital fat stranding and prominent orbital veins. Left cavernous sinus shows increased density suggestive of thrombosis. (C) Plain coronal CT PNS scan showing heterogeneous soft tissue density in the left maxillary sinus, and anterior and posterior ethmoid air cells with sclerosed intercellular septae. (D) Plain sagittal CT orbit and PNS scan showing heterogeneous soft tissue density in maxillary sinus, increased thickness of optic nerve sheath complex, and retro-orbital fat stranding.

{kind=link}
{kind=link}
{kind=link}
Aseptate fungal hyphae and hyphal branches typically at right angles suggestive of Mucor species.
Plain coronal CT of the paranasal sinuses and orbits showed increased soft tissue density in maxillary, anterior and posterior ethmoid air cells (fig 2A–C). Plain axial CT of the orbit showed increased thickness of the optic nerve sheath complex, retro-orbital fat stranding and prominent orbital veins (fig 2D). KOH preparation of the nasal swab (fig 3) showed aseptate fungal hyphae and hyphal branches typically at right angles. Morphology was suggestive of Mucor species.
In view of the imaging findings and the microscopic evidence, a diagnosis of acute invasive mucormycosis with orbital extension was made and the patient was started on intravenous amphotericin B. Endoscopic debridement of the maxillary and ethmoid sinuses was done and the patient’s general wellbeing improved, the periorbital swelling subsided, but the patient was left with blindness in the left eye.
Rhinocerebral mucormycosis is a rare but potentially aggressive and fatal fungal infection.1 It should be considered in all patients with chronic sinusitis, especially in immunocompromised patients. Factors predisposing to invasive mucormycosis include poorly controlled diabetes mellitus, and prolonged corticosteroid treatment. The diagnosis is confirmed histologically by demonstrating tissue invasion and subsequent tissue reaction to the fungi, rather than just the presence of the organism.2 The current treatment strategy involves rapid diagnosis, reversal and stabilisation of underlying medical conditions, systemic antifungals, and appropriate surgical debridement as needed.3
Acknowledgments
All who cared for this patient.
Footnotes
Competing interests: None.
Patient consent: Patient/guardian consent was obtained for publication.