Article Text

Summary
The death of a previously well 13-month-old infant approximately 5 h after his mother contacted the Queensland Nurse led telephone triage call centre ‘13Health’ for advice is the first Australian casualty of telephone triage. Experience from this case and another ‘near miss’ incident Australia highlight the potential of this model of care to harm patients using the service when it attempts to provide health advice compared with health information.
Statistics from Altmetric.com
Background
Telephone triage centres having been introduced in the UK and Australia without any formal evaluation. This case adds to similar cases in the UK to show that telephone triage is potentially dangerous in those patients with emergency medical conditions. I hope that this paper will stimulate a proper evaluation of these services as the fact that this death occurred in Australia in addition to those in the UK highlight the problem lies with the model of care.
Case presentation
The mother of a previously well 13-month-old male infant had a recent chickenpox infection and took her son to his general practitioner (GP) on 9 October 2006 where he received an immunisation against chickenpox. On the night of Saturday 14 October 2006 the infant developed fever of 38.5 °C and mother noted the child did not want to eat, but was drinking, and had a runny nose. The mother, based in suburban Brisbane, called ‘13Health’ for assistance on the morning of Sunday 15 October 2006 as she was concerned about the continuing fever and child's demeanour.
09:32 Mother calls 13Health
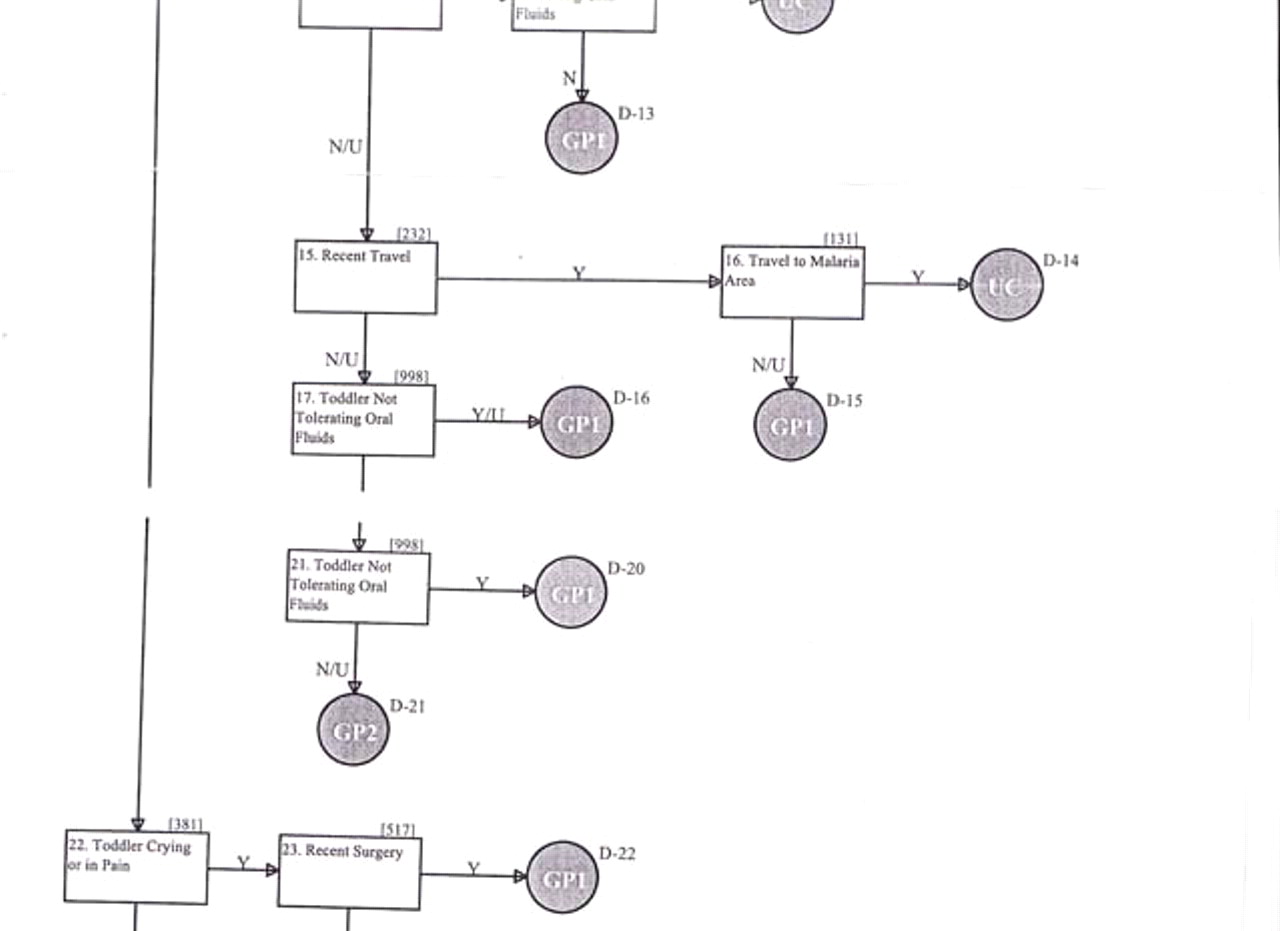
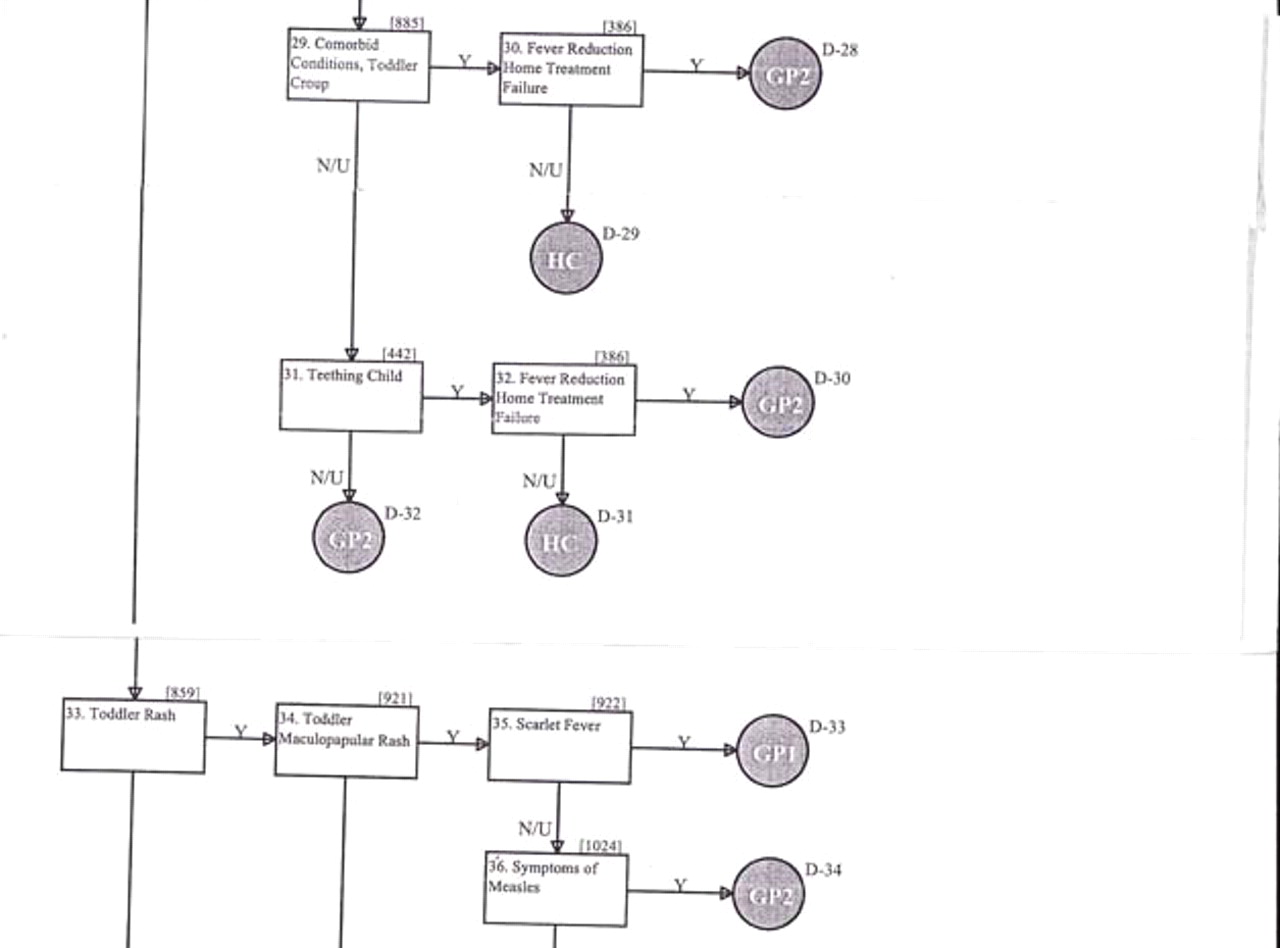
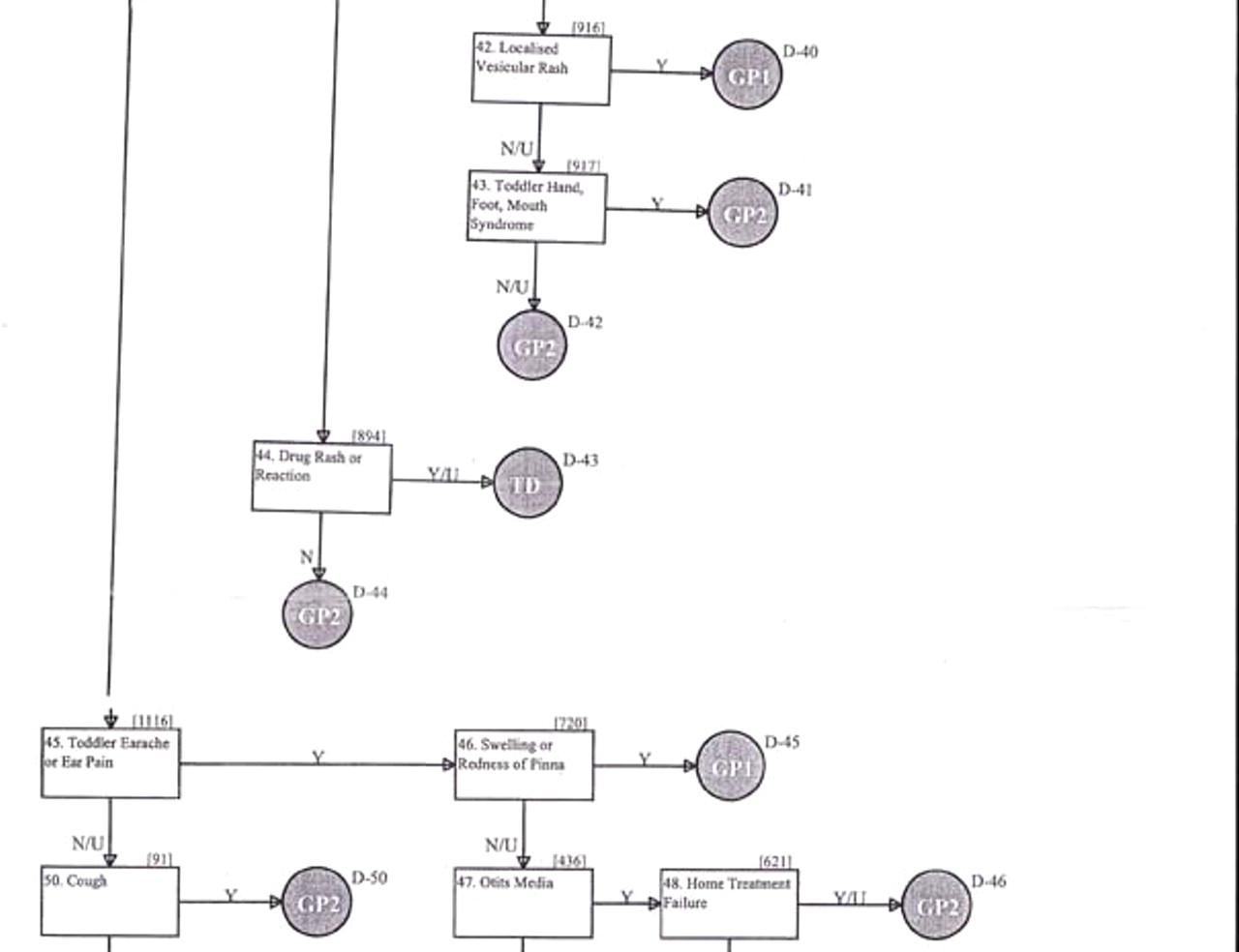
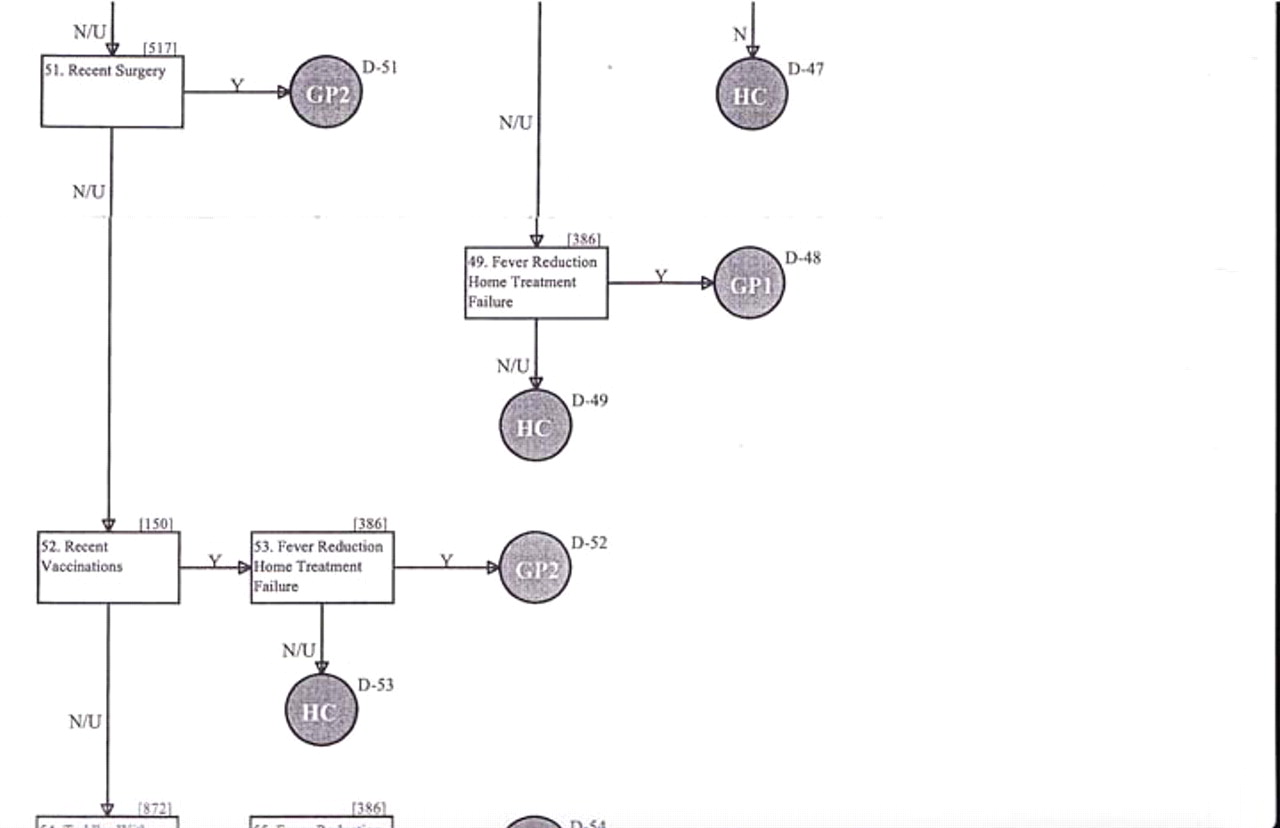
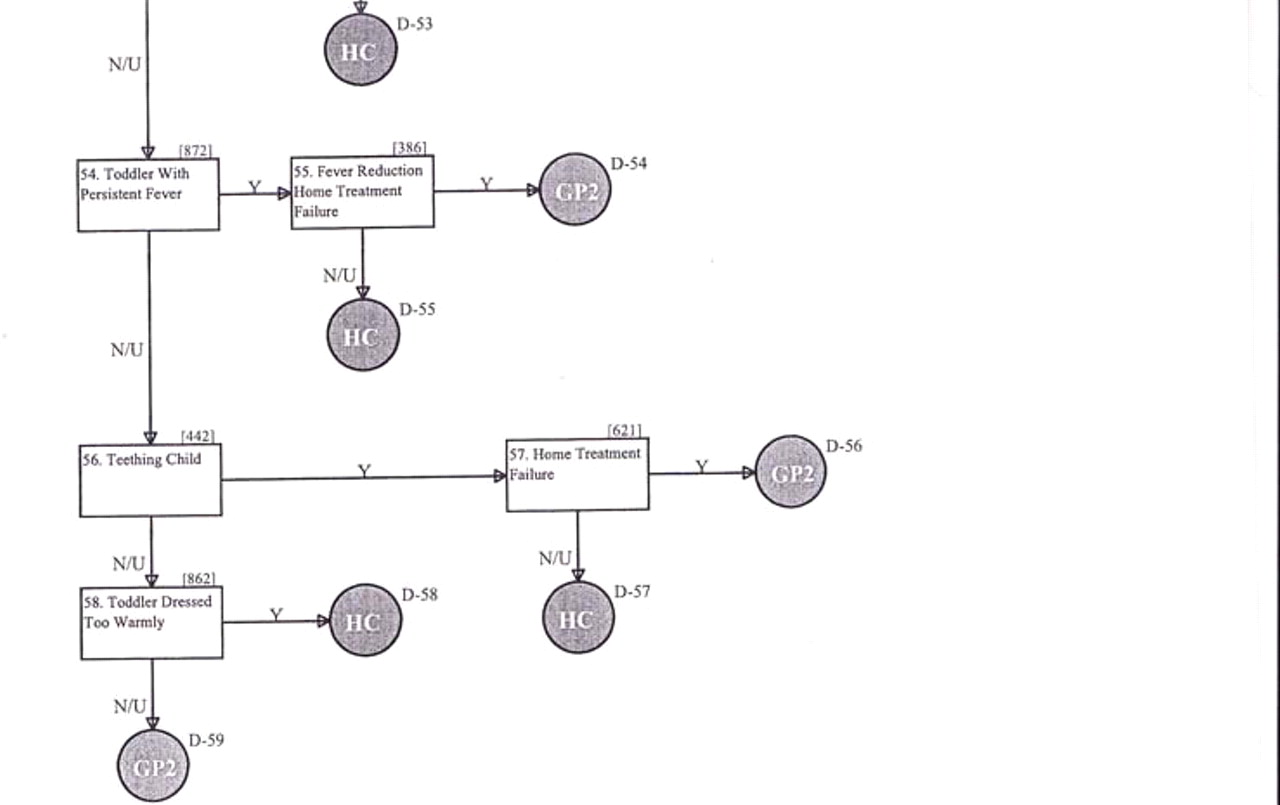
After basic demographic information was obtained the infant's mother was asked a total of 25 complaint specific questions from a 55 question ‘Fever-Toddler’ protocol (figure 1)
09:47 13Health Telephone triage consultation terminated with mother being advised to see her GP in the morning
10:00 Child placed in cot
11:30 Child walks into lounge room
12:00 Child put back to bed
14:39 Child found in cot not moving or breathing. Queensland Ambulance Service called
14:42 Queensland Ambulance Service on scene
15:15 Queensland Police notified of the death









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Fever-toddler protocol as tendered in to the Queensland Coroner.
At autopsy there was patchy congestion and haemorrhage of the lower lobes of both lungs being more prominent in the right lung. Postmortem pulmonary cultures revealed the presence of adenovirus and Streptococcus pneumoniae. There was no evidence of the spread of these organisms in the rest of the body. There was no evidence of chickenpox pneumonia.
Discussion
The death of a previously well 13-month-old infant in 2006 shortly after his mother contacted the Queensland nurse led telephone triage call centre ‘13Health’ for advice is the first Australian death associated with telephone triage. This death was followed by a ‘near miss incident’ in 2007 in another Australian State. In this incident an adult female contacted the service for advice because of fever, myalgia and arthralgia. She was advised to take paracetamol to lower her temperature and go to bed. She called the service again because of increasing pain and was told to take a bath with two tablespoons of bicarbonate of soda for 20 min. After the bath she called an ambulance and was transported to hospital where she was successfully treated for her meningococcal infection.1
Australia is in the process of developing a national telephone triage call centre network by July 2011. This network is based upon the British NHS Direct nurse led telephone triage call centres which were established in 1998. The available literature on telephone triage call centres is confusing as there are several models of care that are either described, or indexed in the medical literature, as ‘telephone triage’. These include nurse led telephone triage call centres using computer prompted protocols, GP supervised nurse staffed call centres and afterhours call centres for either individual or groups of medical practitioners.
In addition there is no distinction made between giving health information by telephone, versus telephone advice as to whether or not to seek medical attention. The risks associated these separate functions are not equivalent as demonstrated by this case. Telephone triage assessments can be further hindered by the normal variations in English language skills and syntax in the community which can impact upon how individual's expresses their symptoms, and their responses to medical questioning. Several life threatening emergency medical conditions in adults and children may initially have vague or non-specific symptoms.2
Telephone triage ignores the important role of visual cues in assigning a triage priority to a patient's symptoms in the emergency department. The correlation between nurses performing telephone versus in-person triage in non-critically ill patients presenting to the emergency department is only 43.1%.3 Even when triage certified nurses used structured triage protocols combined with knowledge of a patient's vital signs the correlation between telephone versus in-person triage was still only 48.8%.3
All available evidence indicates that telephone triage call centres do not decrease, and may even increase emergency department presentations4 in the UK and New Zealand.5
Experience from Australia is that up to 36.4% of calls are advised to see a doctor immediately with 9.1% requiring emergency ambulance transport.6 In addition 5% of callers ignore the call centre advice and subsequently present to the emergency department despite being advised otherwise.7 Problems with telephone triage can arise because patients can be confused about when they need to call for an ambulance directly rather than call a telephone triage call centre.8 Call centre screening introduces avoidable delays for individuals with potentially time critical emergencies which would not exist if patients called for an ambulance directly.9 Delays in the treatment of time critical emergency can result in either potentially preventable deaths or unnecessarily complicate their medical treatment and hospital stay.2 9
Telephone triage call centres are beneficial by providing a single point of contact for health information for members of the community 24 h a day. In addition telephone triage call centres can help direct members of the community to a GP afterhours and allow GPs manage their afterhour's workload. For those hospitals that do not prohibit staff providing telephone advice, telephone triage call centres can provide a standardised advice service that relieves emergency department staff in these hospitals. Improved indexing of medical literature on telephone triage call centres is required to be able to ascertain what impacts telephone triage call centres have on patient outcomes, which has to be an integral consideration of any evaluation of these services.
Learning points
▶ It is dangerous to base health policy on the assumption that patients seeking GP services as being the same as those patients with non-specific symptoms concerned that they may have an emergency medical condition. While there is overlap between these two groups of patients are not identical.
▶ Telephone triage assessments cannot exclude life threatening illness in callers concerned that they may have an emergency medical condition.
▶ Further research is needed to evaluate the impact of telephone triage call centres on the health outcomes of people using the service.
Footnotes
-
Competing interests None.
-
Patient consent Not Obtained.