Article Text

Summary
Cortical representations of the native language and a second language may have different anatomical distribution. The relationships between the phonologic and orthographic forms of words continue to be debated. We present a bilingual patient whose competence in his mother tongue was disrupted following brain ischaemia. Semantic units were accessible only as isolated letters in written as well as oral language presentation. His second language appeared completely unaffected. Whole word system disturbance of both orthography and phonology pathways of the native language could explain this presentation. It is a great opportunity to learn about the language neural network when a bilingual subject presents with brain ischaemia.
Statistics from Altmetric.com
Background
It was in my last year of the residency training programme when I learned that a single patient can change your whole view of neurology. I realised that all my previous studies on aphasia were not enough to explain every patient with language disturbances. Moreover, the relationships between the phonologic and orthographic forms of words continue to be debated. Therefore, a good clinician must assess every patient from a brand new perspective, clear of any preconceived notions. We present a patient with a very atypical aphasic syndrome and try to discuss a theoretical explanation for these symptoms.
Case presentation
A young male, right handed, obese smoker presented with a sudden inability to speak Spanish, his mother tongue. His competence in English, which he had acquired at the age of 7 years, was not affected. As the patient complained about language difficulties only when talking in Spanish, both languages were explored at the same time by a trained bilingual neurologist following a standard order at the emergency room (ER): oral comprehension, repetition, nomination, reading and writing. Every task was asked first in Spanish and then in English, before going on the next issue (table 1). At the nomination task, he was able to spell the name of items in Spanish and, afterwards, say the English whole word (for example, he said L-A-P-I-Z with letters uttered in Spanish and then, “pencil”). This phenomenon was consistent after presentation of five different objects (watch, pencil, glasses, blanket and a glass), without any paraphasia. He could describe the use of these items through pantomime. The patient was able to read letter-by-letter isolated words; although the right item was chosen from several ones presented (the same five ones chosen for the nomination test), the whole word form pronunciation was not achieved in Spanish. His letter-by-letter reading strategy did not depend on explicit letter naming. He was also unable to understand written commands in his native language. The patient was able to write the constituent letters of the names of the items in Spanish, but spontaneous writing was not possible. His score on the National Institutes of Health Stroke Scale was 5 if English language competence was not considered.
Language tasks summary
Investigations and outcome
Emergency magnetic resonance imaging (MRI) (fig 1) was performed. Diffusion weighted images showed left posterior insular and parietal hyperintensities. A perfusion defect corresponding to the inferior division of middle cerebral artery was observed. Thrombolytic therapy was not implemented because the patient completely recovered within 90 min of suffering the stroke. Before complete recovery, our patient presented with phonemic paraphasic errors only when speaking Spanish (as an example, patient said “bolegrafo” instead of “boligrafo”). No additional neurological or general features of clinical interest were present at the time of admission to the ER. Haematological and biochemical measurement revealed a triglyceride value of 246 mg/dl as the only abnormality (laboratory upper limit of normal 180 mg/dl). Erythrocyte sedimentation rate and a workup for connective tissue disorder were found to be normal. Serum RPR (rapid plasma reagin), Lyme disease and HIV infection were discounted, as was abnormality of the coagulation cascade. Detailed ultrasound (carotid colour duplex and contrast transcranial Doppler), transoesophageal echocardiography and Holter electrocardiography did not identify any abnormalities. At discharge, neuropsychological testing identified a mild deficit in the patient’s attention span.
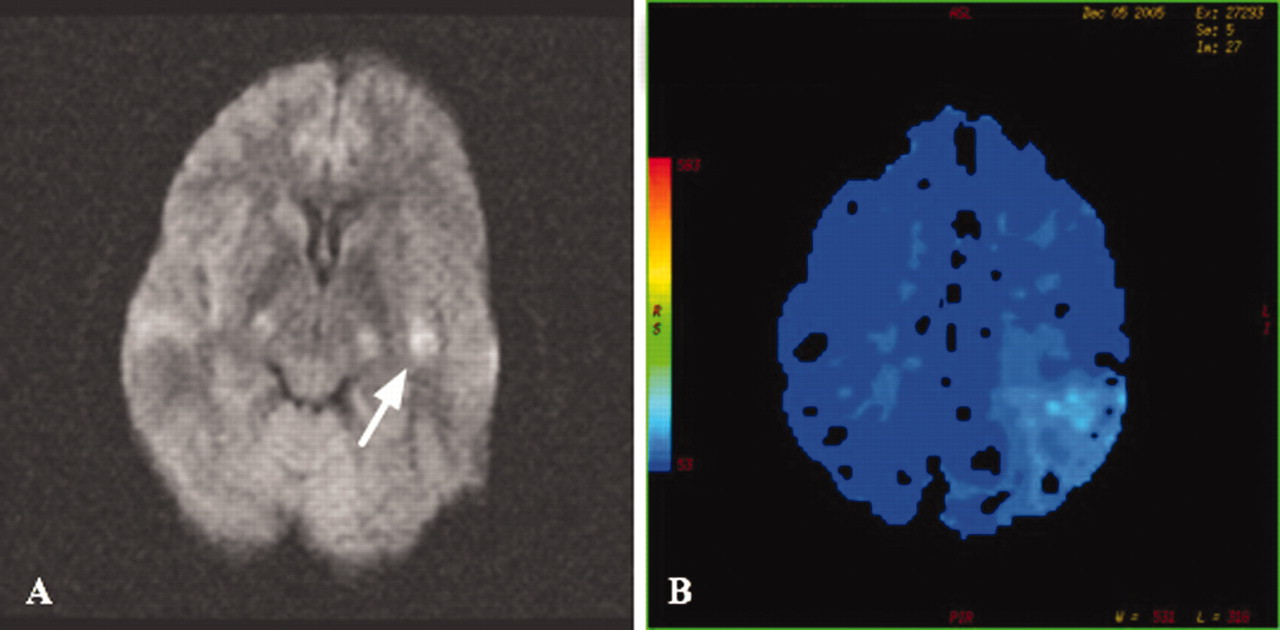
Diffusion (A) and perfusion (B) weighted magnetic resonance imaging 60 min after stroke onset. White arrow shows left posterior insular hyperintensity, with a minor extent then perfusion defect (right side of image).
Treatment
The patient went on a diet and was prescribed anti-aggregation (aspirin 300 mg per day) as a secondary prophylaxis measure.
Discussion
This case is unusual. Formal neuropsychological testing could not be performed, as the acute ischaemic disorder lasted only 90 min. However, even with an incomplete assessment, very useful but cautiously interpreted information was obtained from the emergency room neurological examination.
The cortical representations of a native as well of a second language may be similar in extent but significantly different in anatomical distribution.1 Classical cortical representation of language areas has been redefined by functional techniques during the last few years. Moreover the connections between the phonologic and orthographic forms of words continue to be debated.2
The patient’s mother tongue was affected by the brain ischaemia, but not his second language, English, which was learned in a Spanish school as a foreign language. Formal language studies lasted 11 years. Use of English continued at his work (spoken and written) and when he travelled around the world (at least one journey per year).
This proficiency reached in his second language allowed us to explore disturbances in Spanish with oral commands given in English (for example, “write a sentence in Spanish”). A dissociation between two languages like this one can only be explained if there is at least one language function represented in different cerebral areas. Previous reports on this matter have been published.1,3
At stroke onset, when the patient was asked not to use English, spontaneous propositional and automatic speech were absent. Understanding oral commands and repeating words or sentences when presented in Spanish were not possible. Different items were presented to the patient. He was able to describe their use through pantomime. Instead of retrieving the Spanish whole word, he spelled aloud constituent letters of the Spanish term.
Letter-by-letter reading
As our patient did at the emergency room, it is possible to access semantic units by a letter-by-letter reading strategy.4 This pattern is related to disruption or disconnection of the visual word form area, which may be found at the left inferior temporal region. Dysfunction of this area is also significantly associated with impairment on oral reading, oral naming (visual or tactile input) and written naming.5 This laborious strategy has been reported in bilinguals.6 In this clinical case, native tongue was also the affected language.
As non-words reading was not tested, we are not able to affirm if the patient did not understand written commands because he was not able to read pseudowords, functors and affixes, as described in phonological alexics.7
Writing impairment: phonological agraphia?
When the examiner asked our patient to write the Spanish name of the different items presented, he wrote their correct name letter-by-letter. Phonological agraphia, described elsewhere,8,9 could be a possible explanation for these deficits, but we did not assess if the patient was able to write pseudowords.
A theoretical model
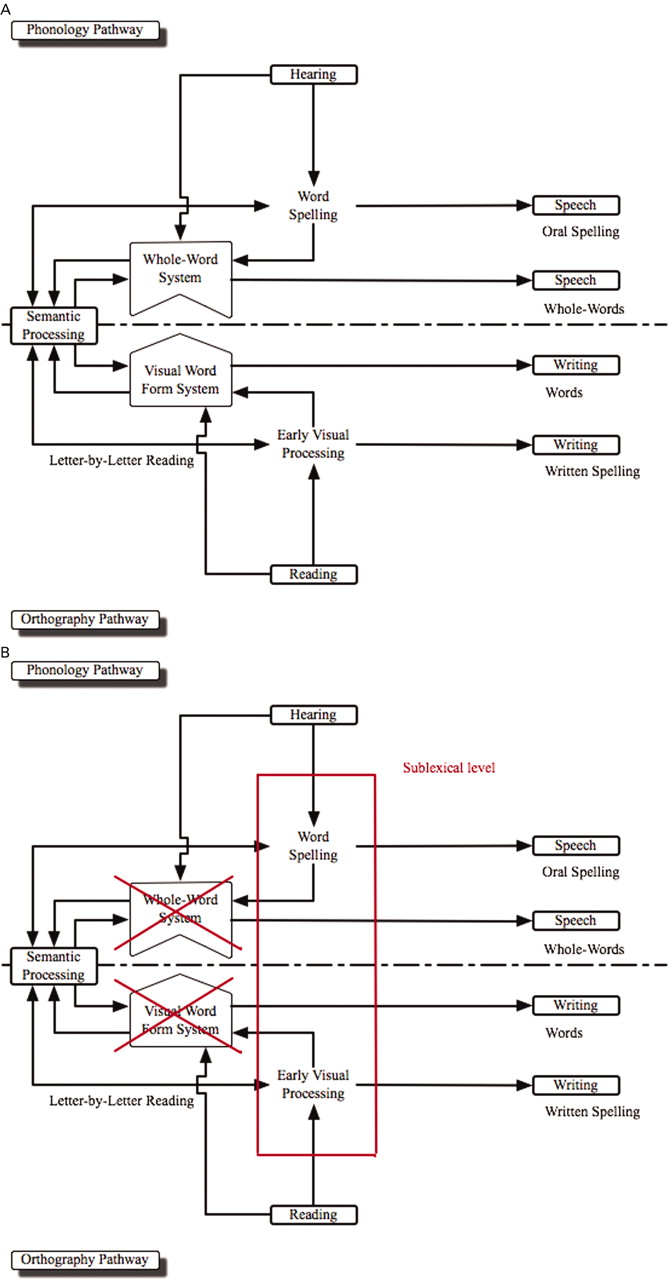
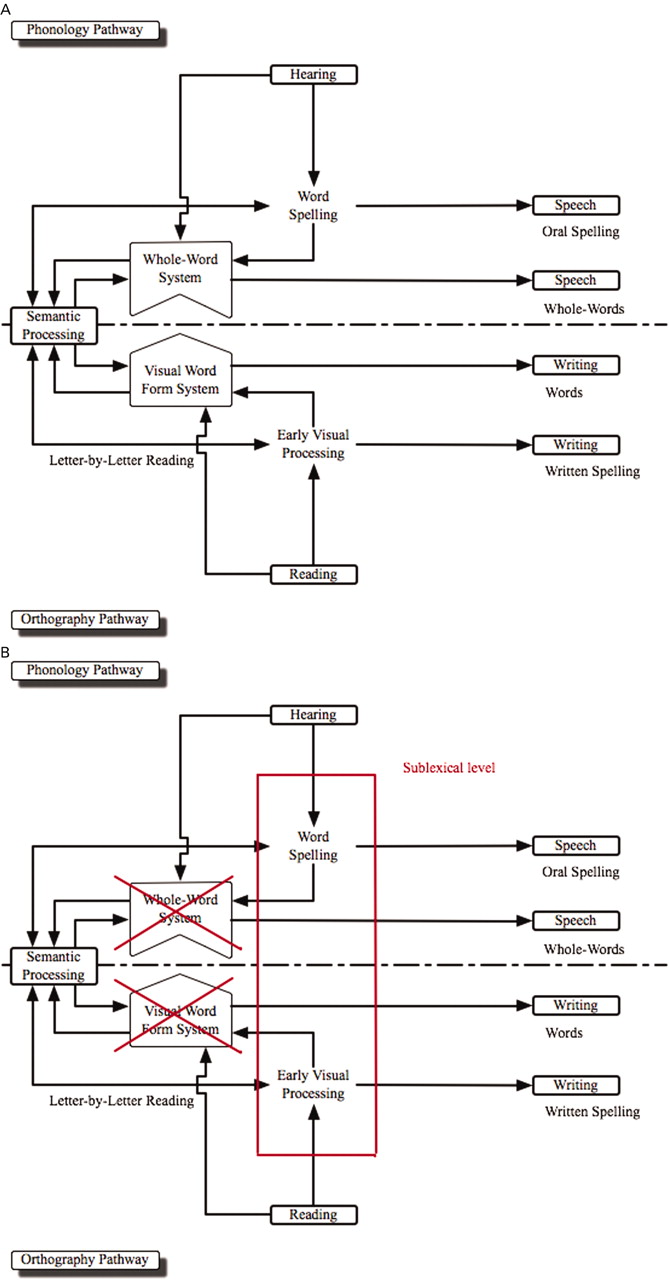
We propose (fig 2A) that the semantic units, if intact, can be accessible to language in two parallel, but separate, levels: the lexical and the sublexical one. At the lexical level, the phonologic form of words functions as a whole unit, and it is related to the orthographic form, which could be represented in the visual word form area; this is consistent with the higher activity found, while phonographic scripts of one language are being read, in and around the supra-marginal and angular gyri in bilateral parietal lobules.10 At the sublexical level there is also a relationship between the phonology and the orthography pathways. The lexical level is a faster way of gaining semantics than the sublexical one, as can be inferred from a functional MRI study published recently11 and which demonstrated that models of word naming and mean time-of-response from the stimulus was shorter for words than non-words, and which do not have a phonologic cortical representation linked to corresponding semantic units. This lexical priming effect is equally strong in second language processing, even for bilinguals who had acquired the second language within a school setting at 10 to 12 years of age.12 As our patient did not appear to have any disturbance with respect to his second language, we were unable to explore this issue further. It is difficult to demonstrate the independence of these two levels in normal and pathological subjects by functional MRI even using non-words or isolated letters as stimuli, because both levels work together and failure may not be absolute. Spanish disturbance in our patient (represented in fig 2B) could be explained by this model. Visual stimuli activated the sublexical level, reaching the semantic units by a letter-by-letter processing strategy. After presentation of different objects, naming was done in Spanish by oral (and written) spelling. So, semantic processing could activate the sublexical level through the phonology (and orthography) pathway. It would have been of great interest to explore what the patient had understood if the examiner had spelled oral commands, just to demonstrate whether the phonology pathway can be activated by an auditory stimulus at the sublexical level.
{kind=link}
{kind=link}
(A) Proposed model of relationships between orthography and phonology pathways at lexical and sublexical levels. (B) Author’s explanation for Spanish disturbance is represented (red crosses indicate lexical level impairment).
This neurological examination could be explained by a reversible lesion in the area responsible for orthography and phonology at the lexical level: the whole word system. To confirm this theoretical model, studies would need to be performed in which a disconnection is induced between different cortical areas, perhaps by electrical interference during routine functional mapping in seizure patients undergoing surgery.
This clinical case is very useful, as the patient could be explored by using his second language. This kind of disturbance may be more frequent than we suppose; monolingual patients present more difficulties to be explored if they do not understand what the examiner means.
Finally, many bilingual patients have come to our emergency room complaining about several difficulties in language. Since our experience with this patient, we keep in mind that deficit does not need to be of the same intensity in every language. Examiners must be very cautious in the emergency room; we presented this clinical case in a session and many experienced neurologists thought this disorder was factitious. Now I teach my residents to try to explain patients’ complaints and symptoms without any preconceived notions.
Learning points
-
There are many aphasic syndromes; many of them are still not well known.
-
Do not doubt a patient’s complaints. Keep an open mind when exploring aphasia.
-
It is a great opportunity to learn about language mechanisms when a bilingual subject presents with brain ischaemia.
Acknowledgments
Dr Garcia and Dr Egido would like to express their gratitude to Dr Barquero, recently deceased. Thanks Marisa for transmitting your love for the patients and your knowledge to us and being our friend.
REFERENCES
Footnotes
Competing interests: None.