Article Text

Summary
Achalasia is characterised by the loss of peristaltic movement in the distal oesophagus and failure of the lower oesophageal sphincter relaxation, which results in impaired oesophageal emptying. We report a case of a 92-year-old frail woman with a history of achalasia, who presented with acute oesophageal obstruction due to impaction of a large amount of food material. She was treated successfully with nifedipine, in combination with Coca-Cola (original product, not sugar free), so avoiding the risks associated with repeated endoscopic intubation and piecemeal removal of the oesophageal content.
Statistics from Altmetric.com
Background
In achalasia, failure of the lower oesophageal sphincter (LES) relaxation may result in food impaction. Many intubations may be required in order to clear the oesophagus, placing the patient at risk of aspiration, trauma or perforation. The use of Coca-Cola in combination with a calcium channel blocker is safe and appropriate first line treatment in the case of elderly or frail patients and where endoscopy is not readily available.
Case presentation
A 92-year-old woman with a 20 year history of achalasia presented with dysphagia, palpitations and restrosternal pain. Two years previously she had been treated for achalasia with Botulinum toxin injection. Upper gastrointestinal (GI) endoscopy revealed a tubular muscular narrowing 2 cm in length at the level of the cardiac sphincter, with a pre-stenotic diverticulum. Biopsies were benign. The stomach and duodenum were normal. She was not willing to undergo treatment and was discharged with advice to consume only blended food. She returned 8 days later complaining of retrosternal pain, heartburn and nausea. On the previous day, she had consumed a rich, non-blended meal comprising fish, potatoes and cheesecake.
Investigations
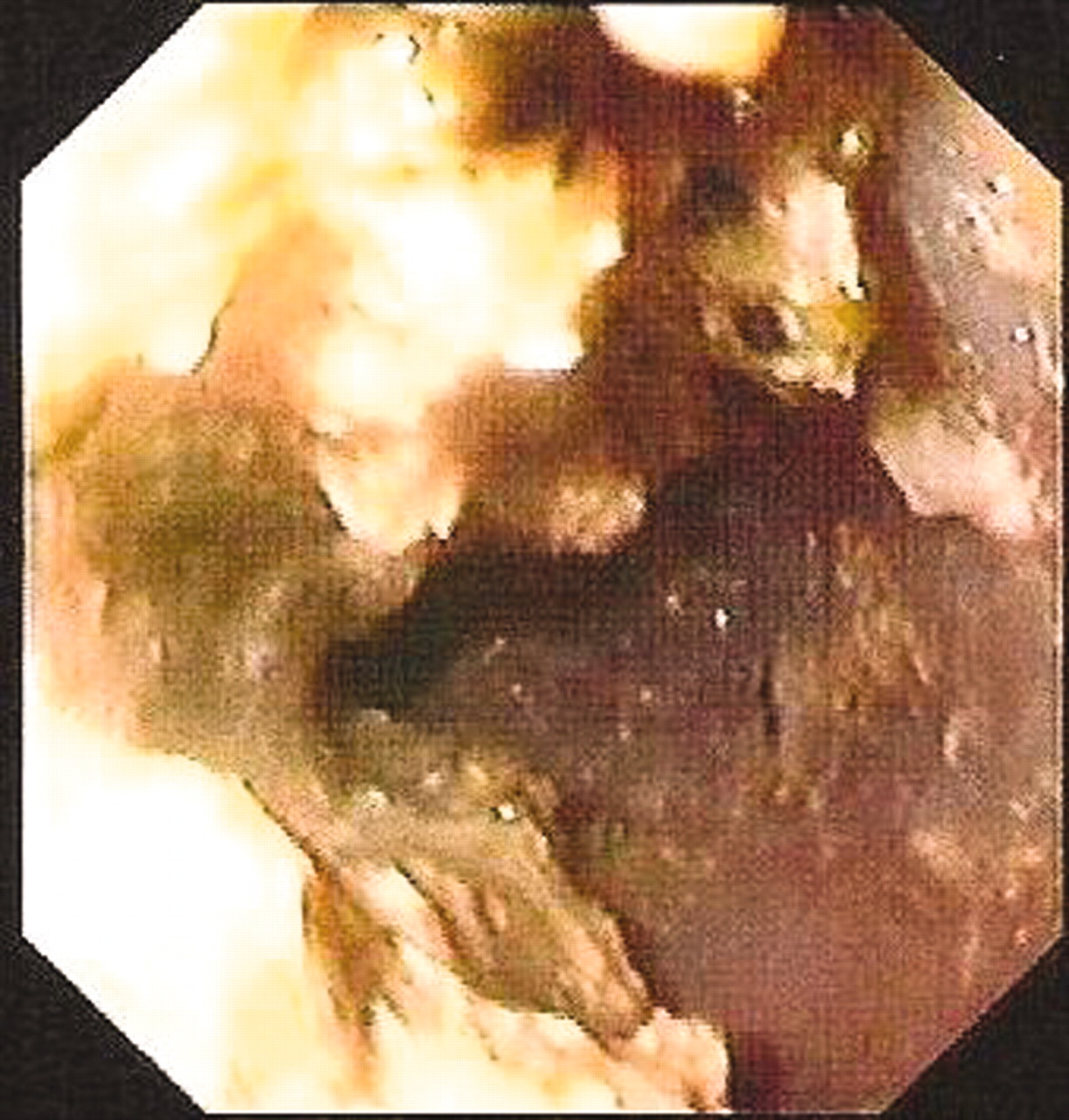
The patient was afebrile and physical examination was unrevealing. Cardiology work-up was negative. Chest radiograph showed no free air in the mediastinum and no signs of aspiration. Upper GI endoscopy revealed mostly soft, paste-like food material as well as solids, completely filling the oesophageal lumen up to a level of 1 cm below the pyriform fossa (fig 1). Endoscopic clearance was deemed hazardous and was not attempted.
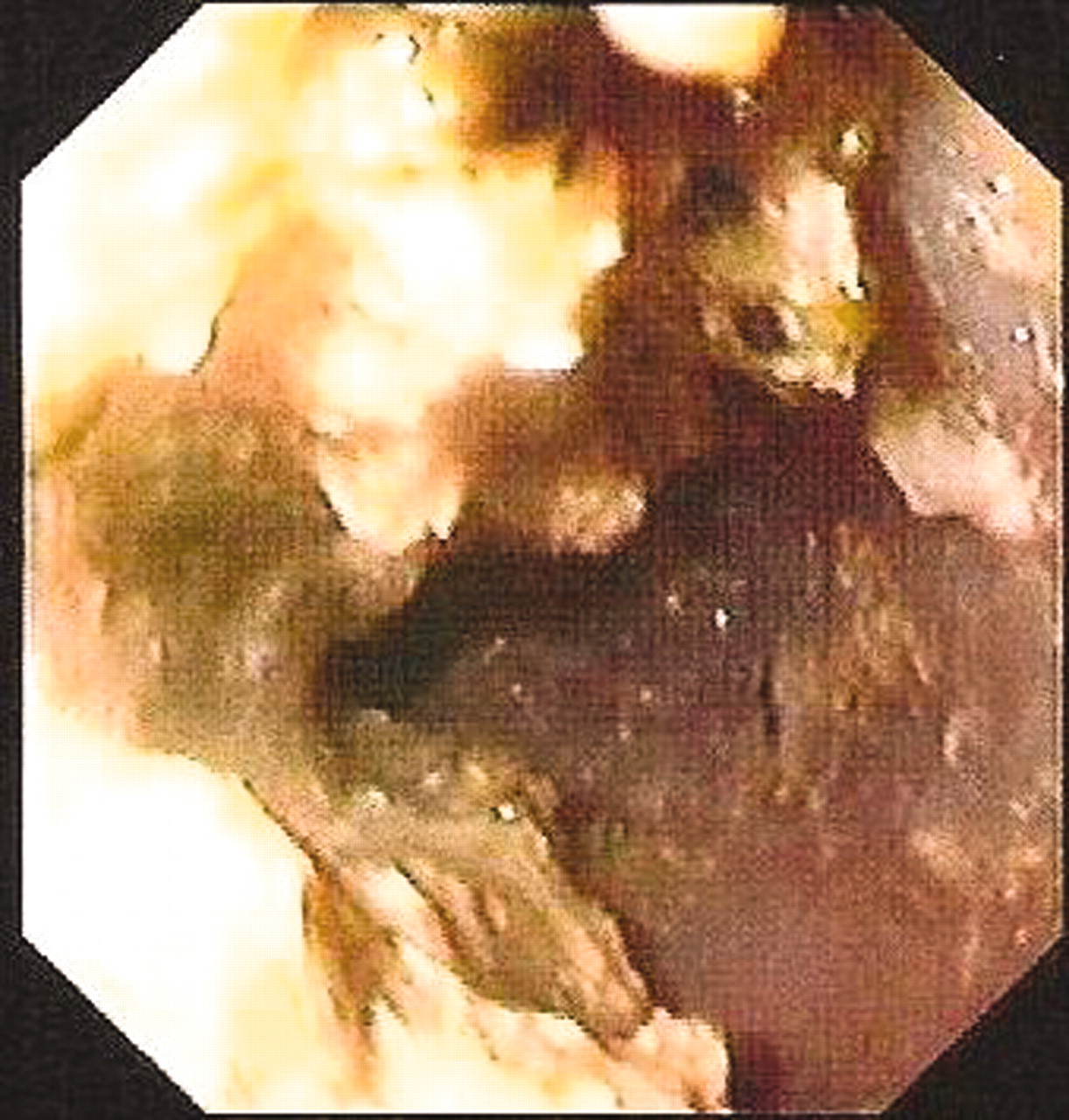
Endoscopy revealing soft, paste-like food material in the oesophageal lumen.
Treatment
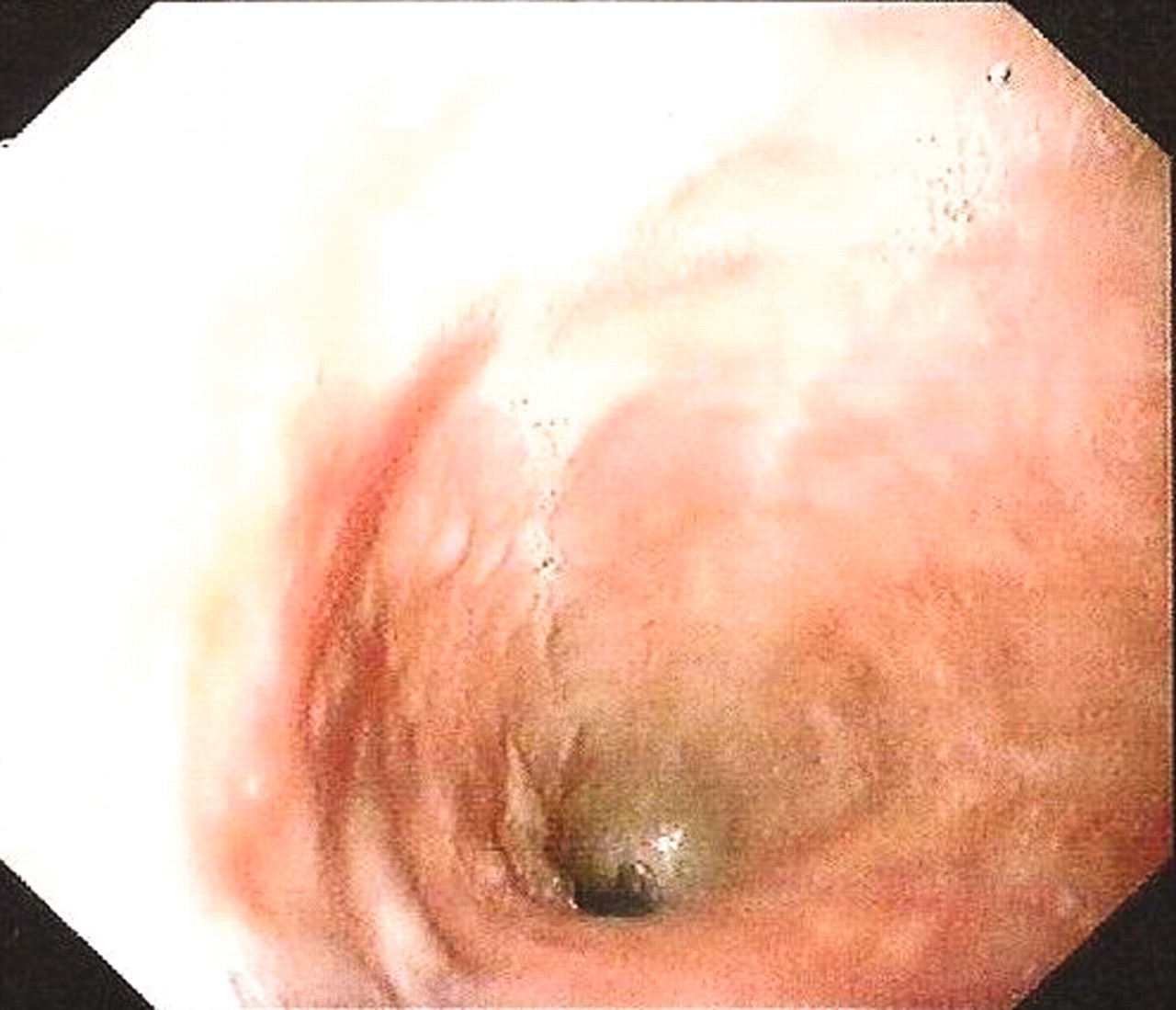
The patient was admitted. Fluids were administered intravenously and nifedipine sublingually at a tolerated (no hypotension) dose of 2.5 mg three times daily. Aiming to liquefy the oesophageal contents, she was asked to drink small amounts of Coca-Cola (original product, not sugar free) starting at 50–100 ml, every 12 h, in small sips, for the first day and increasing to 100 ml every 6 h thereafter, while always remaining in the sitting position. She was allowed to drink only Coca-Cola and no other liquids. She tolerated the intake of Coca-Cola well and did not vomit. Endoscopy after 48 h showed the oesophagus to be completely clear of food residue (fig 2). Botulinum toxin was injected just above the gastro-oesophageal junction (25 units in each quadrant) and she was discharged with advice to consume 1–2 glasses of Coca-Cola daily as a preventive measure.

{kind=link}
{kind=link}
Endoscopy after 48 h, showing the oesophagus to be completely clear of food residue.
Outcome and follow-up
At 4 months follow-up the patient was well with no further episodes of food impaction.
Discussion
In achalasia, failure of the LES to relax may result in food retention in the oesophagus, even of soft, paste-like food. While endoscopic retrieval of the material is usually safe for small amounts of food, in the case of our patient, soft and solid food completely filled the whole length of the oesophagus resulting in poor visibility. In addition, many intubations and retrievals would have been necessary to clear the oesophagus, so placing the patient at repeated risk of aspiration, trauma or perforation. Pushing the material through the LES is hazardous (especially in the presence of an oesophageal diverticulum as in this case), and best avoided.1 In view of these considerations, and being aware of the potentially reversible nature of the obstruction in achalasia by the use of a calcium channel blocker, we used nifedipine for cardiac sphincter relaxation, along with the liquefying action of Coca-Cola.
Calcium channel blockers, as well as nitrates, phosphodiesterase inhibitors and glucagon, are smooth muscle relaxants, which reduce the LES pressure and may be used as a supportive therapy for patients with achalasia.2,3 The use of carbonated beverages to treat food obstruction was first described in 1981 by Felson in a patient with achalasia and stenosing cancer.4 Others reported the use of carbonated soda water to dislodge oesophageal foreign bodies5 and the use of Coca-Cola in the management of bolus obstruction in benign oesophageal stricture.6 Fizzy drinks and sodium bicarbonate solutions7 penetrate the bolus and are thought to disintegrate it by releasing carbon dioxide, which in turn triggers relaxation of the LES so that the liquified bolus enters the stomach. Other methods that have been suggested to relieve acute food obstruction include the topical use of proteolytic enzymes such as papain.8 In our case we used solely Coca-Cola.
We advocate the cautious use of Coca-Cola in combination with a calcium channel blocker as safe and appropriate first line therapy in the case of elderly or frail patients, and where endoscopy is not readily available. It should also be used in all cases of achalasia where the amount or nature of the food impacted in the oesophagus is such as to render endoscopic removal hazardous. Others have also reasonably indicated that endoscopic clearance of the oesophagus is best reserved as second line therapy.4
Learning points
-
In achalasia of the cardia, endoscopic clearance of impacted food material may be hazardous.
-
Lower oesophageal sphincter relaxation with nifedipine in combination with Coca-Cola may safely resolve food impaction.
-
Coca-Cola ± nifedipine may be appropriately used as first line therapy in the care of elderly or frail patients, when endoscopy is not readily available, and where many endoscopic intubations would be required to achieve clearance.
Footnotes
Competing interests: None.
Patient consent: Patient/guardian consent was obtained for publication.