Article Text

Statistics from Altmetric.com
Description
Spinal schwannomas are peripheral nerve sheath tumours that account for approximately 30% of extramedullary spinal cord tumours, found predominantly in sensory roots of the spinal nerve and occasionally in motor roots.1 Most spinal schwannomas are small, well encapsulated and intradural. However, 10–15% extend through the dural root sleeve as dumbbell tumours with both intradural and extradural components, and approximately 2–10% are entirely extradural.2
According to Seppälä et al, the incidence of spinal schwannomas varies between 0.3 and 0.4 cases per 100 000 persons per year with no statistical difference in prevalence between males and females.3 Although their malignant potential is low, they can be locally destructive if allowed to progress.
We report an atypically large extradural spinal schwannoma, which was initially discovered on chest x-ray during work-up for flu-like symptoms and episodes of difficulty in breathing. Interestingly, our 76-year-old male patient was free of neurological symptoms and had an otherwise insignificant past medical history.
CT scans of the thorax showed this lesion to be paravertebral in location and associated with erosion of the posterior right ribs and a thoracic vertebral body. Subsequent MRI scans (figure 1) demonstrated that the tumour was approximately 6×8×8 cm in size (figure 2) and extended from the T5/6 to T8/9 disc with intraspinal extension through the intervertebral foramen at the T8/9 level. A core biopsy was obtained through CT guidance and the histological findings of the tissue revealed typical features of a benign schwannoma with both hypercellular Antoni type A and pauci-cellular Antoni type B tissue.
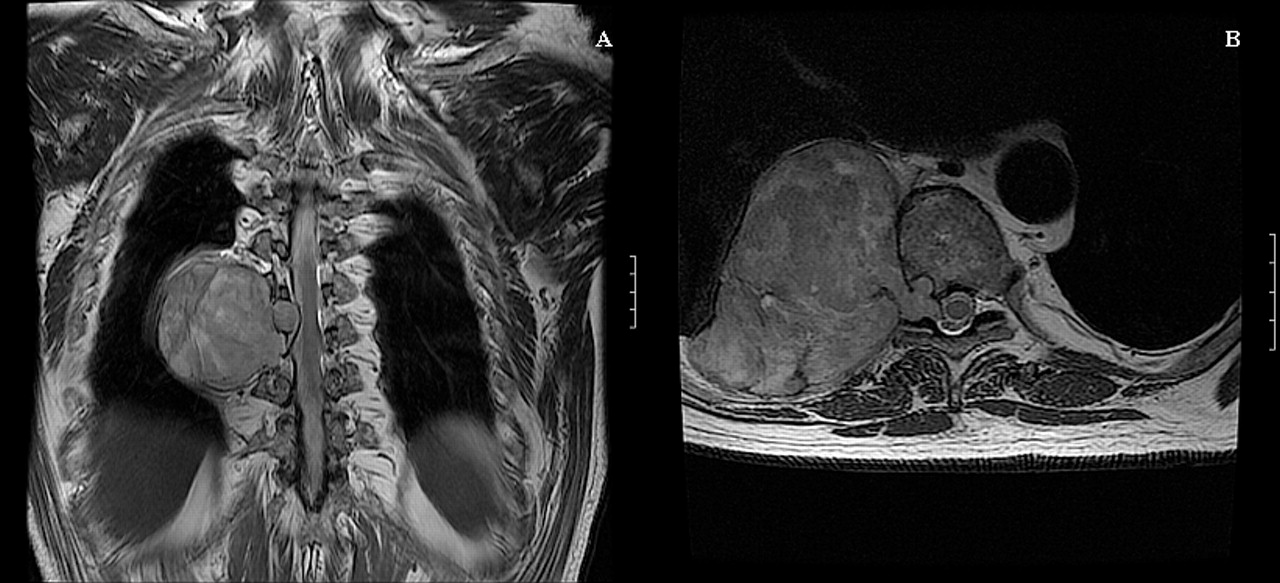
(A) T2-weighted coronal MRI showing the tumour extending from approximately the T5/6 disc to the T8/9 disc. (B) T2-weighted axial MRI showing infiltration of the tumour into the spinal canal.

{kind=link}
{kind=link}
Tumour 6×8×8 cm in size.
Like most other extramedullary neoplasms, spinal schwannomas usually produce local segmental deficits before distant neurological deficits appear. Cervical lesions can produce weakness, fasciculation and atrophy of hand muscles. Thoracic lesions can produce band paraesthesia or Horner's syndrome, while lumbosacral lesions can produce lower extremity weakness as well as bladder and bowel symptoms.4
After a careful preoperative evaluation, it was decided that surgery should be performed in a joint effort with the cardiothoracic team. Intraoperatively, the tumour was seen to be densely adherent to the spinal nerve roots, lung, oesophagus and ribs. It appeared that the tumour was extradural in origin and there was no evidence of intradural extension. The tumour was successfully removed from these structures.
In summary, spinal schwannomas may present as unrecognised slow growing tumours. Their deceptive benign classification should not lead to underestimation of their potential size and the damage they can do to surrounding structures. An accurate preoperative diagnosis is important so that proper management can be prepared.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.