Article Text

Statistics from Altmetric.com
Description
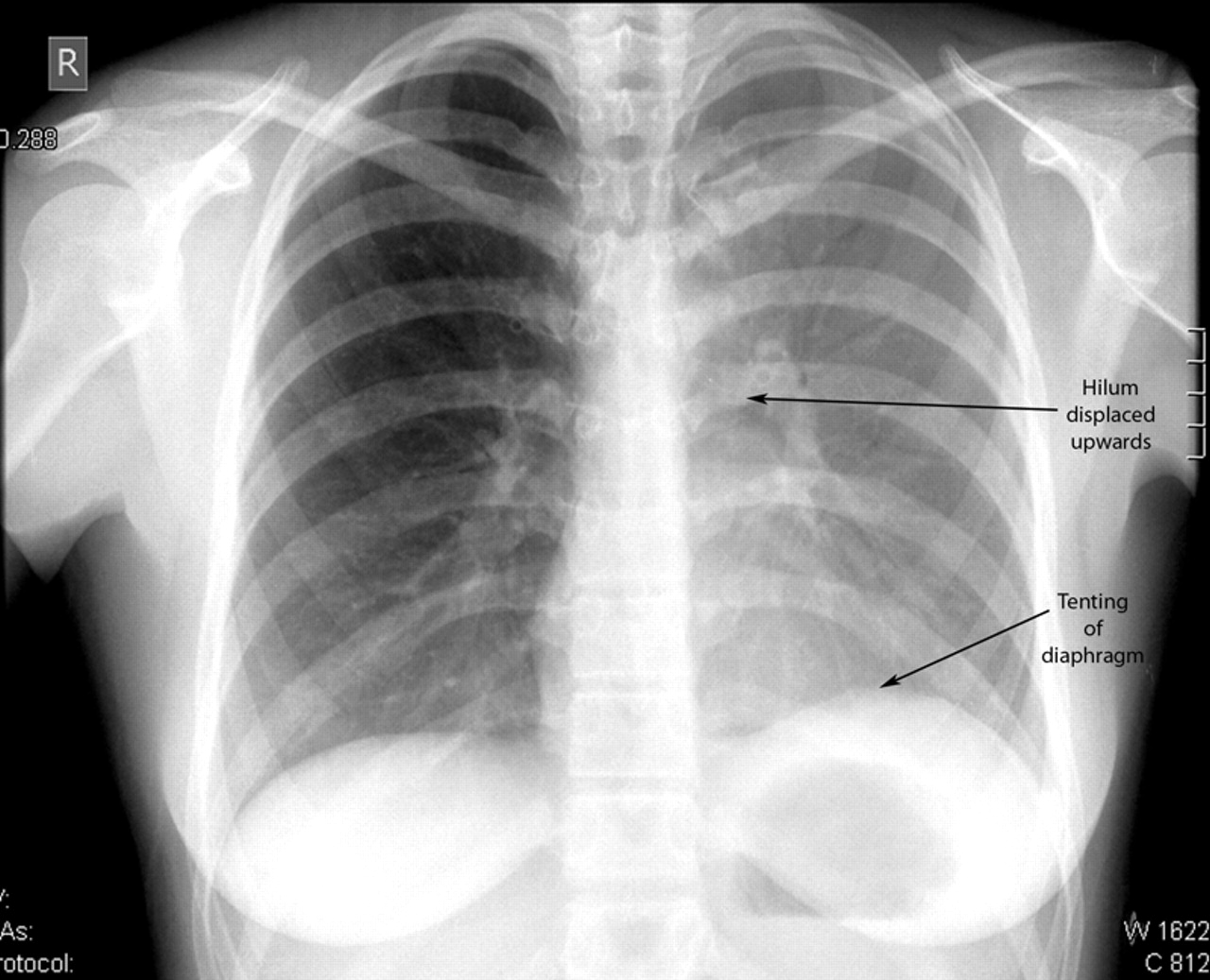
A 16-year-old, non-smoking, girl presented with a 1-week history of productive cough. She was diaphoretic, had no evidence of rigors, temperature was 37.4 °C, respiratory rate was 18/min, oxygen saturation on room air was 94% and blood pressure was 110/50 mm Hg. Auscultation of her chest was normal. Investigations showed a C reactive protein of 116.9 mg/litre and arterial blood gas on room air PaO2 of 10.2 kPa. Initial chest x-ray (CXR) showed diffuse haziness of the left hemithorax with air bronchograms adjacent to the left hilum and upward displacement of the left hilum and diaphragm (figure 1). A diagnosis of pneumonia with left upper lobe collapse was made. She was started on antibiotics and had chest physiotherapy. CT of the thorax was considered but not performed due to clinical improvement and her young age. Follow-up CXR 3 days later showed re-expansion of the left upper lobe with improvement in lung volume; a dense left upper lobe consolidation with prominent air bronchograms (figure 2). Left upper lobe collapse can present with a ‘veil-like’ opacity of the left lung field with elevation of the left hilum and hemidiaphragm.1 This is because the left upper lobe collapses anteriorly. There may also be an area of crescentric lucency between the mediastinum and the atelectatic upper lobe. This is known as the Luftsichel sign.2 3 This represents the upward expansion of one of the segments of lingular lobe. Other potential aetiologies of such findings on CXR include cystic fibrosis and asthma, but our patient had no evidence or history of either.
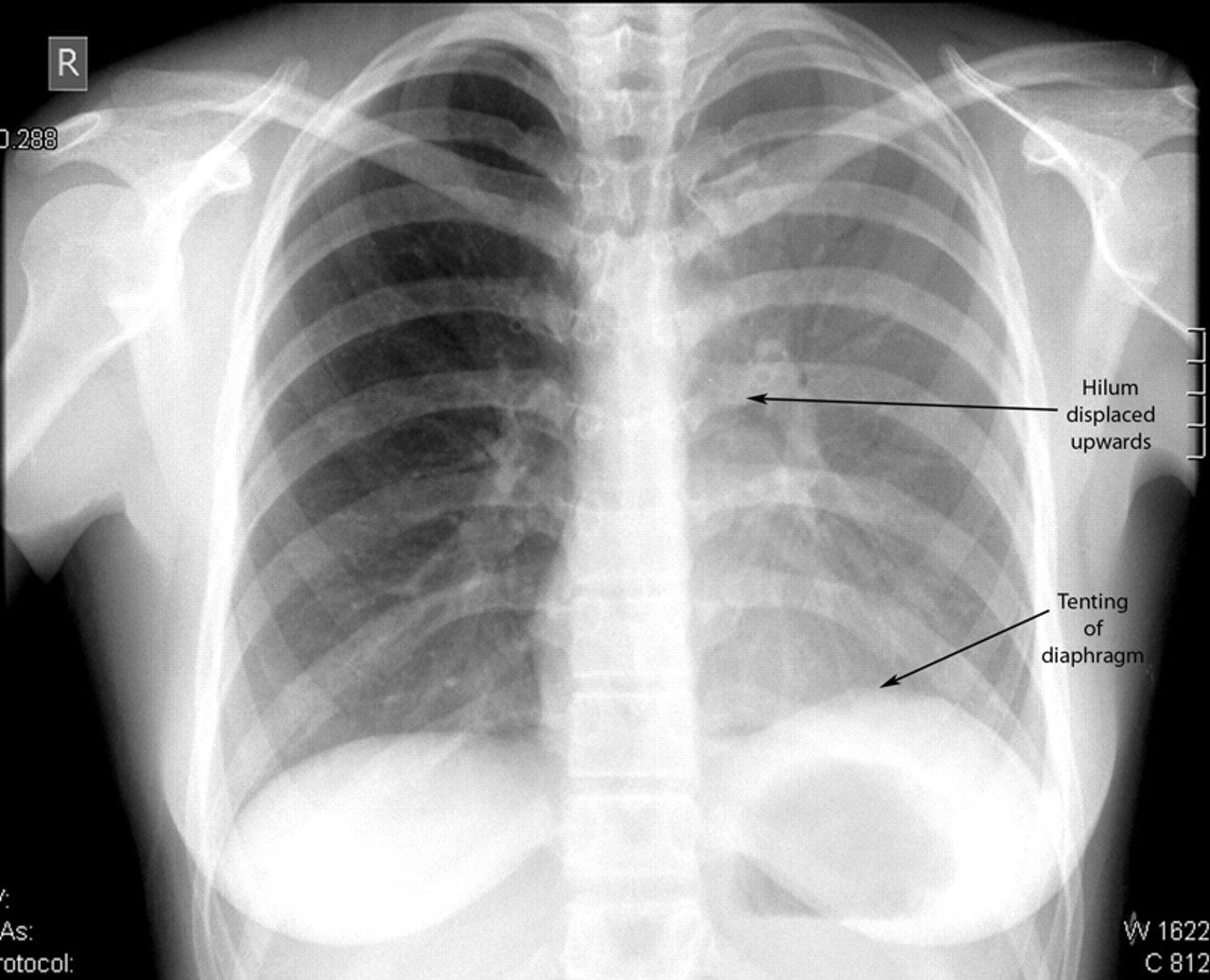
Initial CXR showing the veil-like opacification of the left hemithorax with upward displacement of the left hilum and minor tenting of the left hemidiaphragm.

{kind=link}
{kind=link}
Follow-up CXR demonstrating some re-expansion of the left upper lobe. Prominent air bronchograms are noted.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.