Article Text

Statistics from Altmetric.com
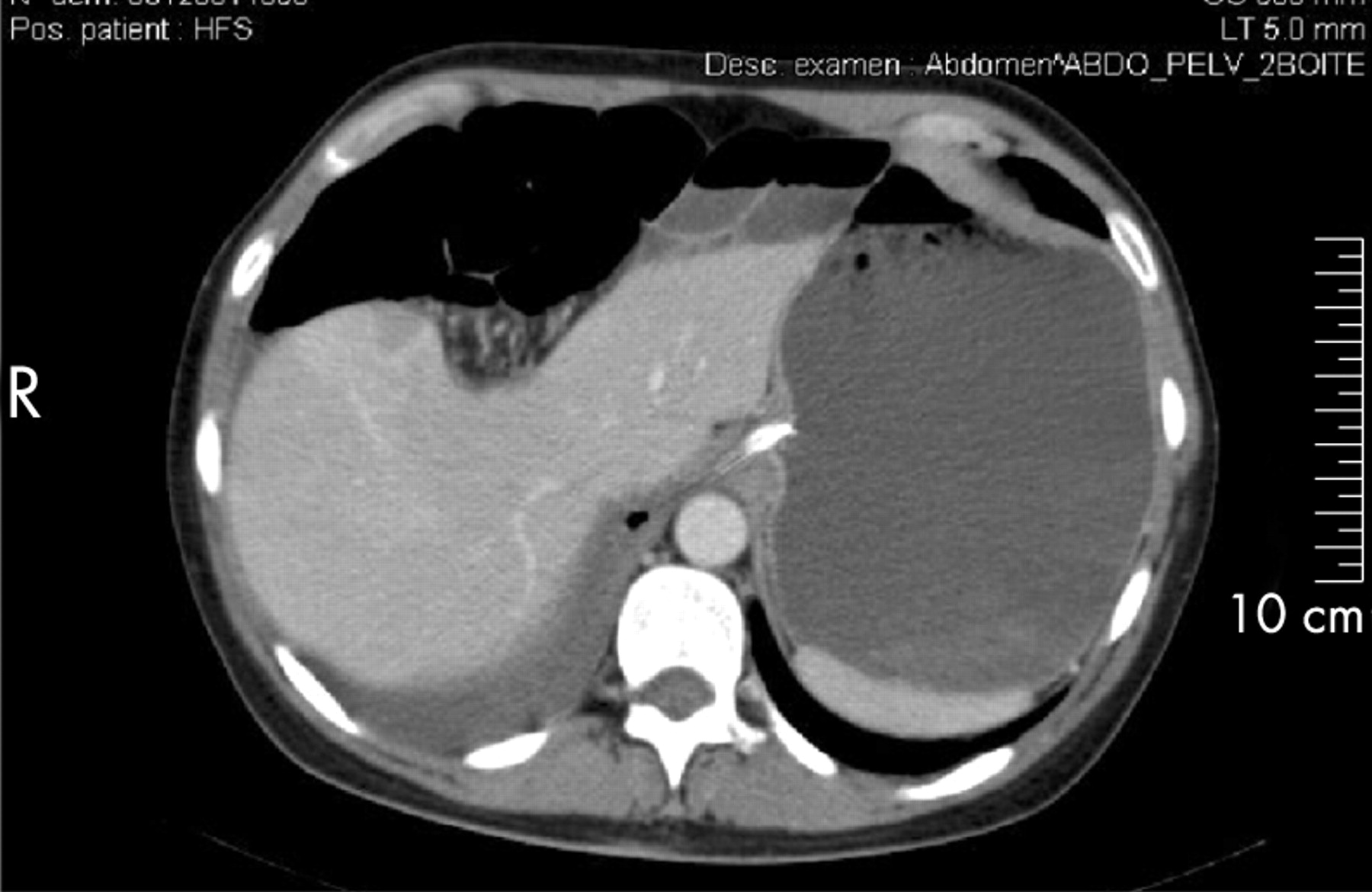
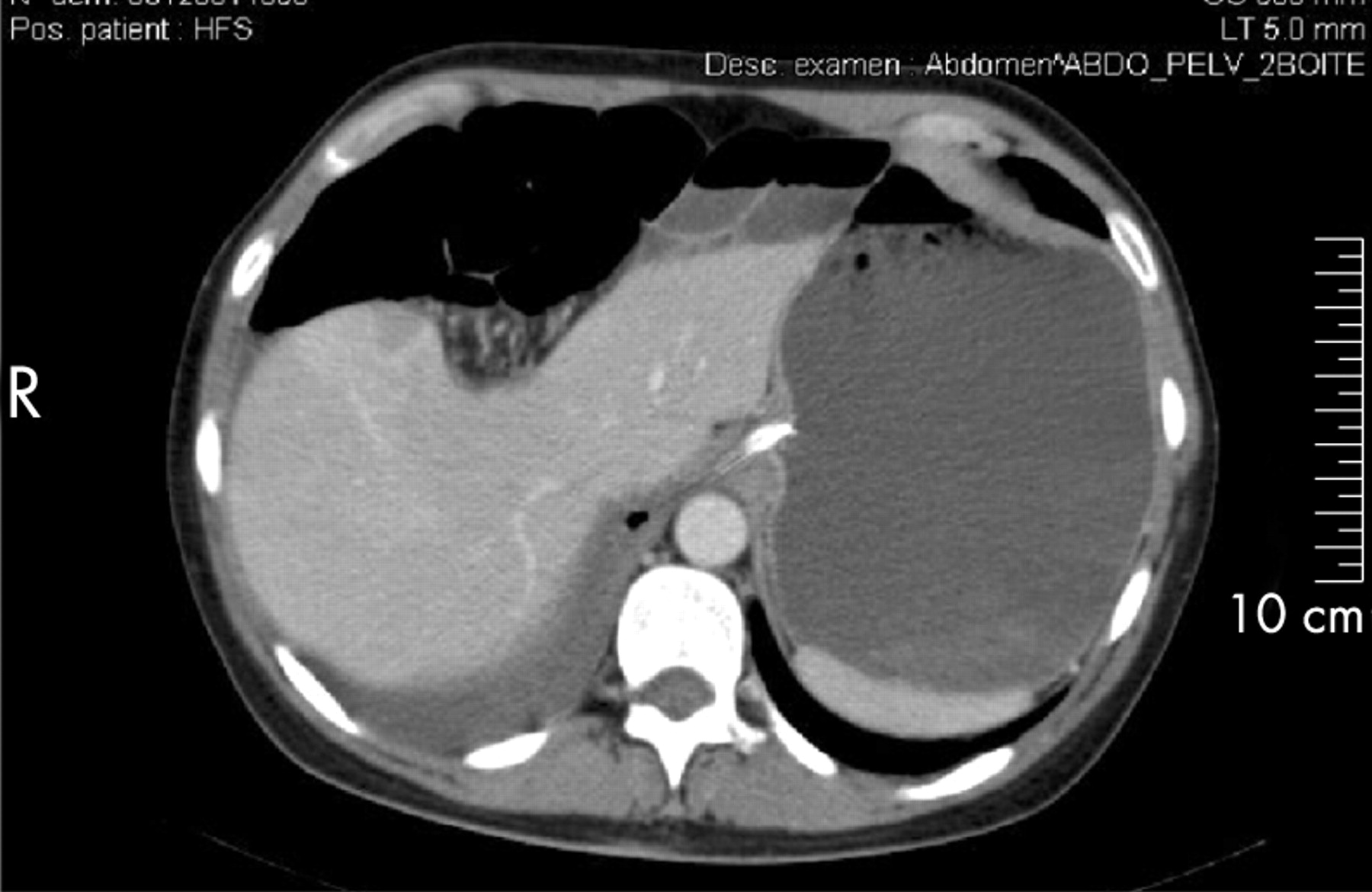
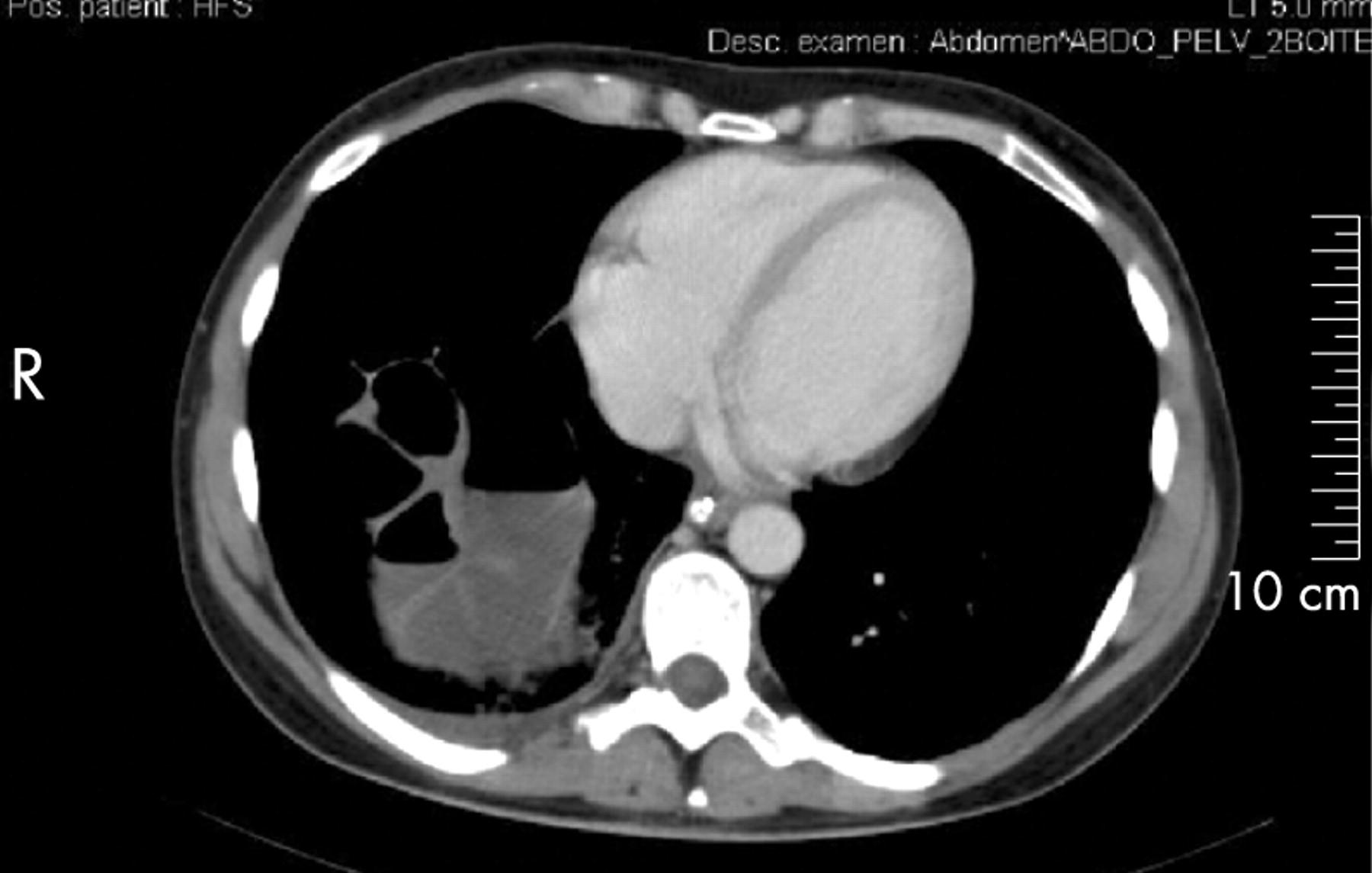
A 40-year-old woman presented to our emergency department with an acute 4-hour history of central abdominal pain associated with nausea and vomiting. She had no past medical or surgical history but had undergone a second uncomplicated delivery 15 days previously. Her body mass index was in the normal range. The patient had marked distension and pain of the abdomen without evidence of peritoneal irritation. A posteroanterior chest radiograph (fig 1) revealed an elevation of the right part of the diaphragm with abdominal gas interposition between the liver and the diaphragm. A CT scan showed that the transverse colon was interposed between the liver and diaphragm but also revealed an incarcerated right-sided Bochdaleck hernia (figs 2 and 3). A laparotomy was performed and confirmed the diagnosis of strangulated Bochdaleck hernia. The herniated small intestine was pushed back into the peritoneal cavity and the defect of the diaphragm was closed. The patient recovered completely from surgery.


{kind=link}
{kind=link}
{kind=link}
Hepatodiaphragmatic interposition of the bowel was first described by Demetrius Chilaiditi in 1910.1 It is often an incidental finding, which can exist temporarily or permanently, and can be mistaken for pneumoperitoneum. This radiographic entity, known as Chilaiditi’s sign, has been associated with various abdominal complications including gastric and colonic volvulus, intestinal obstruction, suprahepatic appendicitis and (as in this case) diaphragmatic hernia. The condition is then called Chilaiditi’s syndrome. The appearance of the CT scan is the critical factor in the therapeutic decision-making process.
Acknowledgments
This article has been adapted from Hivert B, Der Sahakian G, Claessens Y E, Randone B, Afanou G, Allo J C. Chilaiditi’s sign or Chilaiditi’s syndrome in the emergency department Emergency Medicine Journal 2008;25:87