Article Text

Statistics from Altmetric.com
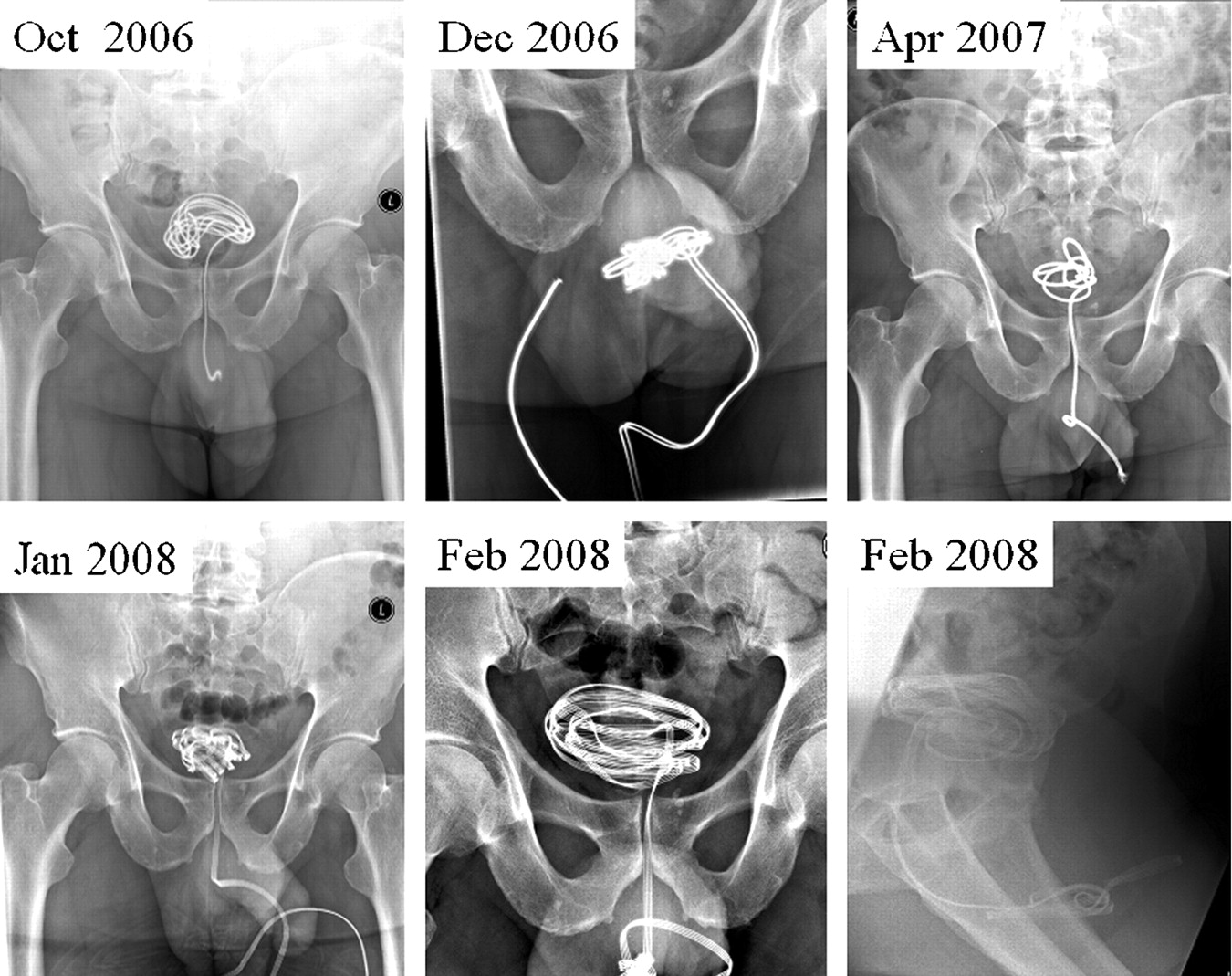
We present the case of a 52-year-old male patient with a history of bipolar disorder, borderline personality disorder and self-mutilation under the influence of drugs and alcohol. This patient was known to have alcoholic liver cirrhosis and seizures, and was frequently seen at the urology department of our university hospital due to the insertion of an electrical telephone cable into his bladder (fig 1).
{kind=link}
Each time the phone cable was inserted in such a way that it formed a knot in the urethra or in the bladder and had to be removed surgically. During the last two episodes there was extended urethritis in combination with necrosis of the proximal urethra.
Starting during a period of transition from one psychiatric caregiver to another, this patient inserted different types of phone cables into his urethra under the influence of cocaine and alcohol. This resulted in five operations between January 2005 and January 2008.
Self-insertion of intra-vesical foreign bodies due to psychiatric disorders has been described previously in the literature.1,2
In this case, the repetitive insertion of a foreign object into the bladder and urethra can be identified as severe auto-mutilation. There is serious danger of complications such as cystitis, necrosis and stricture of the urethra, bladder perforation, etc.
This patient has proved that urological removal of the telephone cable does not cure the fundamental problem. Clinical considerations also depend on broad psychiatric differential diagnoses from body dysmorphic disorder to factitious disorder or malingering, or from borderline personality disorder to schizophrenia. In cases such as that presented here, a multidisciplinary approach should be followed in which the psychiatrist and the patient’s general practitioner are involved in order to reduce the chance of repetition.
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication.