Article Text

Summary
Acute abdomen with multicystic ovaries as a presenting manifestation of juvenile primary hypothyroidism is rare. Appropriate diagnosis and levothyroxine treatment is rewarding and avoids inadvertent surgery. We present three such cases.
Statistics from Altmetric.com
CASE PRESENTATION
Case 1
An 18-year-old girl, with a 4 year history of oligomenorrhoea, presented with progressively increasing abdominal distension for 4 months and a dull aching abdominal pain for the previous 20 days. She had menarche at 15 years of age. Ultrasonography revealed bilateral multicystic ovaries (fig 1), and a contrast enhanced computed tomography (CECT) scan confirmed the finding with a suspicious solid mass in the right ovary (14×9×9 cm and 11×8×5 cm, right and left ovaries, respectively). Her serum CA 125, β-human chorionic gonadotrophin (hCG) and α-fetoprotein were within normal limits. Fine needle aspiration from the mass revealed haemorrhagic fluid. Because of the possibility of malignancy, the patient underwent right salpingo-oophorectomy. Intraoperatively, right ovarian torsion was observed. Histopathology showed haemorrhagic necrosis with no viable tissue. Postoperatively the abdominal pain subsided but the abdominal distension persisted, and she continued to remain amenorrhoeic. Six months later on the work up for amenorrhoea, her serum thyroid stimulating hormone (TSH) and prolactin were reported to be high and the patient was referred to us.
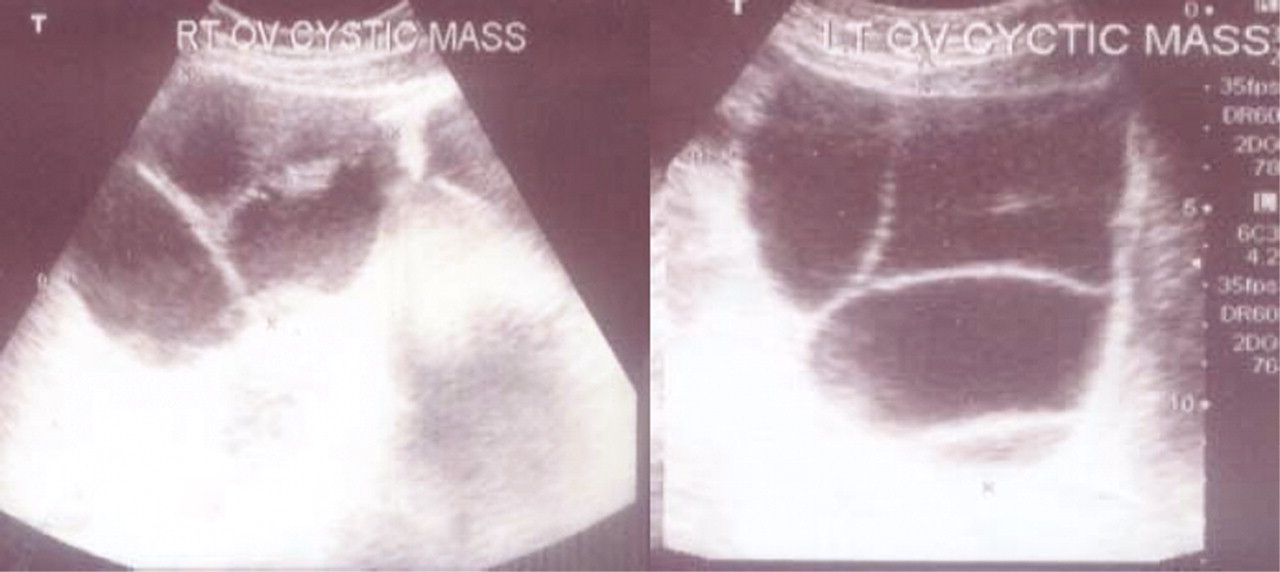
Ultrasonography of the pelvis showing bilateral huge multicystic ovaries.
On examination, her height was 137 cm (<−3SD), weight 44 kg, pulse 80/min, and blood pressure was 120/78 mm Hg. She was pale, and had periorbital puffiness and coarse dry skin. The thyroid gland was not palpable and there was no lingual thyroid. Her secondary sexual characteristics status was B5A2P3 (Tanner stage V) and she had expressive galactorrhoea. Systemic examination revealed delayed deep tendon reflexes. Abdominal examination showed a midline scar and a huge palpable mass of about 10×10 cm in the left iliac region extending to the hypogastrium and umbilical region; the lower margin of the mass was not discernible.
On investigation, her haemoglobin was 9.3 g/dl, serum total triiodothyronine (T3) 0.3 nmol/l (normal range (NR) 1.2–3.0 nmol/l), total thyroxine (T4) 7.7 nmol/l (NR 61.8–163.4 nmol/l), TSH 1104 μU/l (NR 0.27–4.2 μU/l), anti-TPO (thyroid peroxisomal antibodies) 286.4 IU/ml (N <34 IU/ml), cortisol (8 am) 319 nmol/l (NR 171–536 nmol/l), prolactin 154.9 μg/l (NR 4.7–23.3 μg/l), luteinising hormone (LH) 0.436 IU/l (NR 2.4–12.6 IU/l), follicle stimulating hormone (FSH) 9.27 IU/l (NR 3.5–12.5 IU/l), and 17-β oestradiol 4315 pmol/l (NR 45.9–642.4 pmol/l), suggesting that she had spontaneous ovulation. Visual acuity and visual fields were normal. Her bone age was 14 years. Ultrasonography of the pelvis showed an enlarged left ovary with well defined cystic lesions with multiple septations which were confirmed on CT scan (14×12×11 cm), while the right ovary could not be seen (fig 2). Magnetic resonance imaging (MRI) in the sellar area showed a 1.3×2 cm sized lobulated intensely enhancing mass. The patient continued to be treated with levothyroxine and the dose was increased to 150 μg. At 3 months of follow-up, the abdominal mass disappeared clinically and a CT scan showed regression of the left ovarian mass (fig 3).

Contrast enhanced computed tomography (CT) scan of the pelvis showing an enormously enlarged left ovary, while the right ovary is not visible.

{kind=link}
{kind=link}
{kind=link}
Contrast enhanced CT scan of the pelvis showing regression of the ovary after 3 months of levothyroxine replacement therapy.
Case 2
A 19-year-old girl presented 3 years previously with acute abdominal pain for which she underwent laparotomy. On exploration, a huge multicystic left ovary was found and removed. However, a diagnosis of hypothyroidism was not established for the next 2.5 years when she started complaining of headache, followed by bilateral progressive loss of vision. A CECT of the head showed a 40×45 mm enhancing mass in the sellar area with suprasellar extension. She was referred to our institute with a diagnosis of non-functioning pituitary tumour. She attained menarche at the age of 16 years and 1 year later had cessation of menses. She also had a history of lethargy, fatigue and body aches. On examination, her height was 127 cm (<−3SD), weight 33 kg, pulse rate 94 beats/min and blood pressure 114/70 mm Hg. She was pale, had periorbital puffiness and coarse dry skin. Her secondary sexual characteristics status was B5 A2P2 (Tanner stage V) and she had expressive galactorrhoea. Systemic examination revealed delayed deep tendon reflexes and the fundus showed bilateral optic atrophy. Abdominal examination revealed an ill defined firm mass in the right iliac and hypogastric region.
On investigation, her serum total T3 was 0.7 nmol/l, total T4 25.6 nmol/l, TSH 357.7 mU/L, cortisol (8 am) 450 nmol/l, prolactin 128 μg/l, LH 0.5 IU/l, FSH 9.7 IU/l, and 17-β oestradiol 73.4 pmol/l. 99mTc scan was suggestive of a sublingual thyroid. Anti-TPO antibody titre was insignificant. Bone age was 14 years. CECT of the abdomen showed a huge right multicystic ovary, whereas the left ovary could not be seen. She was started on levothyroxine therapy, after which she had a remarkable improvement in myxoedematous manifestations, vision and regression of the multicystic ovary by >90% at 6 months.
Case 3
A 16-year-old girl had menarche at the age of 12 years followed by secondary amenorrhoea. She also had progressive abdominal pain and distension, weight gain, facial puffiness, lethargy and fatigue. On evaluation, she was diagnosed as having bilateral huge multicystic ovaries and she underwent bilateral ovarian cystectomy. Concurrently, she was also diagnosed with primary hypothyroidism (total T3 0.64 nmol/l, total T4 30.9 nmol/l, TSH 84 mU/l) and was treated with levothyroxine. However, she continued to remain amenorrhoeic for almost 3 years and was referred to us for further work up. On examination, her height was 143 cm (<−3SD), weight 47 kg, pulse 82 beats/min, and blood pressure 118/80 mm Hg. She was pale and did not have a goitre. Her deep tendon reflexes were normal. Her secondary sexual characteristics status was B5 A1P1 (Tanner stage V). On investigation her serum total T3 was 2.6 nmol/l, total T4 191.5 nmol/l, TSH 0.01 mU/l, and anti-TPO was 33.0 IU/ml as she was on 150 μg of levothyroxine. However, her serum LH was 47.3 IU/l, FSH 33.0 IU/l, and 17-β oestradiol <18.35 pmol/l, indicating that she had undergone bilateral oophorectomy.
DISCUSSION
These case studies amply illustrate two important issues: (1) a lack of appreciation of the salient features of chronic thyroxine deficiency in patients with longstanding juvenile primary hypothyroidism; and (2) its recognition as a cause of acute abdomen in these patients.
The salient features of longstanding juvenile hypothyroidism include deficient linear growth, delayed puberty, peripubertal menorrhagia, goitre and non-specific symptoms such as weight gain, lethargy, fatigue and constipation.1 Rarely, they may present as a sellar mass due to thyrotrophe cell hyperplasia2 and precocious puberty.1 The causes of acute abdomen in patients with hypothyroidism include acute cholecystitis with cholelithiasis,3 multicystic ovaries with or without ovarian torsion,4 and intestinal obstruction and sometimes with megacolon.5 These manifestations are more prevalent in children and rarely occur in adults with primary hypothyroidism.4 Multicystic ovaries usually present with an abdominal mass and, if left unattended and undiagnosed, can become very large, reaching up to the hypogastrium as was observed in two of our patients. An acute abdomen as a presenting manifestation in patients with multicystic ovaries is either due to ovarian torsion or sometimes due to acute enlargement caused by haemorrhage into the cyst, as seen in one of our patients. On many occasions inadvertent surgery has been performed, as also happened in our patients. The other causes of multicystic ovaries during peripubertal age are hyperprolactinaemia, thyrotoxicosis, late onset congenital adrenal hyperplasia, and sometimes adrenocortical tumours.
The pathophysiology of multicystic ovaries include altered LH/FSH ratio in favour of FSH due to decreased gonadotrophin releasing hormone (GnRH) pulse generator activity and decreased clearance of FSH.6,7 Diminution of negative feedback by thyroxine leads to increase in TSH and FSH as both are glycoprotein hormones, and TSH acting on the FSH receptor on the ovary —a phenomenon called “specificity spillover”—also contributes to multicystic ovaries.8
The differential diagnosis of ovarian masses in adolescents includes arrhenoblastoma and theca cell tumours, which are usually small, unilateral and present with virilisation. Epithelial tumours, which are usually large and bilateral, are uncommon in this age group. These tumours are usually associated with increasing concentrations of specific serum tumour markers which were normal in one of our patients.
The most common cause of primary hypothyroidism in children is Hashimoto’s thyroiditis,9 which may or may not be associated with goitre at presentation. Ectopic thyroid as a case of hypothyroidism is less common at this age as was seen in one of our patients.
Very large multicystic ovaries, a result of advanced disease, are usually associated with thyrotrophic cell hyperplasia which manifests as headache and visual field defects, as was seen in one of our patients, or it may sometimes be asymptomatic as well.2 The association of both simply represents the long duration of the disease.
The time course of regression of multicystic ovaries after optimal levothyroxine therapy varies between 3–6 months in most case studies.10,11 High dose levothyroxine replacement therapy (300 μg) has been used in patients with vision threatening thyrotrophic cell hyperplasia.12 However, such data for enormously enlarged multicystic ovaries are not available. We observed a remarkable reduction in ovarian size after 3–6 months of levothyroxine replacement therapy in our patients.
Conclusion
Multicystic ovaries as a presenting manifestation of juvenile primary hypothyroidism is rare and represents advanced disease. Appropriate diagnosis and levothyroxine replacement therapy is effective and prevents inadvertent surgery. Therefore, serum TSH should be measured in every adolescent with menstrual irregularities.
LEARNING POINTS
-
Multicystic ovaries as a presenting manifestation of juvenile hypothyroidism is rare and represents advanced disease.
-
Appropriate diagnosis and levothyroxine replacement therapy is effective and prevents inadvertent surgery.
-
Serum TSH should be measured in every adolescent with menstrual irregularities.
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication