Article Text

Summary
Mycobacterial spindle cell pseudotumour (MSCP) has been reported in various sites, including skin, lymph nodes, bone marrow, lung and spleen. Cutaneous lesions are extremely rare and the differential diagnoses include various spindle cell lesions. Literature review shows that this lesion has preponderance for upper limb involvement and occurs largely in immunosuppressed individuals. We report a case of MSCP of the skin due to atypical mycobacterium and discuss the risk of misdiagnosis as a sarcoma.
Statistics from Altmetric.com
BACKGROUND
Mycobacterial spindle cell pseudotumour (MSCP) is a spindle cell proliferation resembling a mesenchymal tumour and the proliferating cells are found to contain mycobacteria. Although MSCPs have been reported in various sites (lymph nodes, bone marrow, skin, lung and spleen), most of the cases reported have been lymph nodes. A review of the literature showed only five cases of cutaneous MSCP described to date. The important of this lesion is that it could mimic some spindle cell tumours. We report a case of spindle cell pseudotumour of the skin due to atypical mycobacterium.
CASE PRESENTATION
A 43-year-old man presented with a 2-week history of right wrist swelling associated with weakness of the medial two fingers. There was no history of past medical illnesses. Clinical examination showed a swollen wrist, fingers and palm. There was numbness over the medial one and half fingers and the medial side of the palm. The clinical provisional differential diagnosis was malignant histiocytoma.
INVESTIGATIONS
Blood investigations revealed a normal white cell count (6.0×103/UL), haemoglobin level (13.3 g/dL) and platelet count (210×103/UL). The Venereal Disease Research Laboratory (VDRL) test and assays for HBsAg and HIV were negative. MRI of the right wrist and hand showed extensive inflammation in the subcutaneous tissue and muscle. The radiological findings were suggestive of infection.
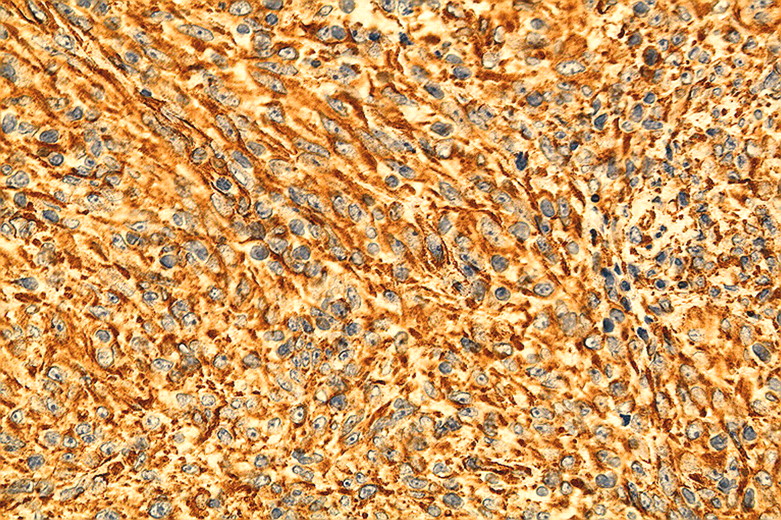
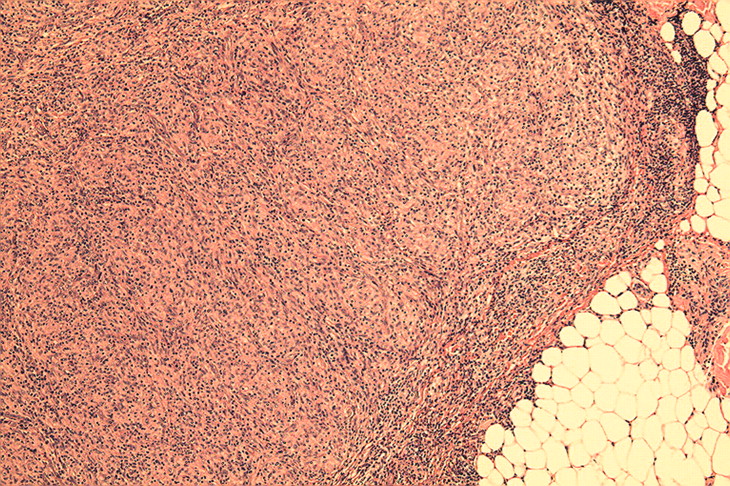
At operation, there was a vague mass lesion compressing the ulnar nerve and covering the tendon, which was impossible to completely excise. On microscopic examination, a spindle cell proliferation was seen, nodular on low power examination (fig 1). A background of lymphoplasmacytic infiltrate was present. The spindle cells display large vesicular nuclei, finely granular chromatin and occasional prominent nucleoli with ample cytoplasm (fig 2). At medium power examination, these spindle cells formed vague granulomas. There was no evidence of caseous necrosis or giant cell formation. Zeihl Neelsen stain revealed numerous acid fast bacilli within the spindle cells. The spindle cells were positive for CD68 (fig 3) and vimentin (fig 4). Atypical mycobacterium was cultured (mycobacterium other than tuberculosis). The patient was treated with rifampicin, dapsone and minocycline.
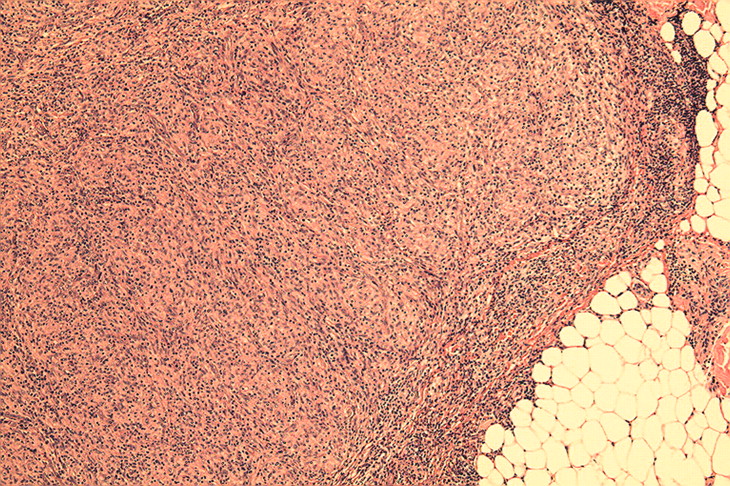
Spindle cell proliferation forming nodular appearance (H&E ×40).

Spindle cells display large vesicular nuclei with ample cytoplasm (H&E ×200).

Spindle cells show cytoplasmic positivity toward CD68 (×200).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Spindle cells show cytoplasmic positivity toward vimentin (×200).
DISCUSSION
Mycobacterium spindle cell pseudotumor is reported to be commonly associated with immunocompromised states, such as HIV infection, cardiac transplant, patients with diabetes and patients treated with prednisolone.1 Our patient tested negative for HIV infection and is not on immunosuppressive agents. In the literature, these patients are aged from 34–58 years old (average 43.3 years). All lesions occurred mainly in the upper limb with predominance for right-sided involvement. The male to female ratio was 5:1. (table 1)
Reported cases of spindle cell pseudotumours of the skin associated with mycobacteria (updated from Shiomi et al)1
In 1963, Wade described variant form of lepromatous leprosy in which a spindle cell proliferation was prominent.6 This histoid leprosy may be regarded as a form of MSCP as on microscopic examination, histoid leprosy has a characteristic storiform spindle cell proliferation. There is usually epidermal atrophy with a subepidermal Grenz zone and a well-circumscribed dermal area of closely packed spindle-shaped histiocytes forming whorls.7
Various Mycobacteria have been isolated as causative agents for MSCP, including Mycobacterium avium-intracellulare, M kansasii, M gordonae, M tuberculosis and M leprae. It is important to recognise the lesion as infective and not neoplastic in nature as the management differs. MSCP should be considered in the differential diagnoses of a spindle cell lesion in the skin, especially in immunosuppressed patients. Other histological mimics worthy of considering are other spindle cell lesions such as dermatofibroma (benign fibrous histiocytoma), neurofibroma, nodular fasciitis, xanthogranuloma, dendritic cell tumour and Kaposi’s sarcoma. When the lesion has a prominent inflammatory component, inflammatory myofibroblastic pseudotumour is an important consideration. The fact that this lesion is also positive for vimentin may be a diagnostic trap and result in a diagnosis of sarcoma. Histiocytic markers such as CD68 and MAC387 may be helpful and Zeihl Neelsen stain follow by culture study will confirm the diagnosis.
The granuloma formation is associated with a delayed-type hypersensitivity reaction initiated by CD4+ T cells. The cytokine responsible for the activation and transformation of macrophages into epithelioid cells is believed to be interferon-γ released from CD4+ T cells.8 Some authors have concluded that the pathogenesis of mycobacterial spindle cell pseudotumour involves a complex host–microorganism interaction.3
In conclusion, if spindle cell lesions are occurring, especially in immunocompromised patients, mycobacterial spindle cell pseudotumour should be considered as one of the differential diagnosis.
LEARNING POINTS
The majority of mycobacterial spindle cell pseudotumours (MSCPs) occurs in immunocompromised individuals.
Histological mimics of MSCP include dermatofibroma (benign fibrous histiocytoma), neurofibroma, nodular fasciitis, xanthogranuloma, dendritic cell tumour, Kaposi’s sarcoma and inflammatory myofibroblastic pseudotumour.
Histiocytic markers such as CD68 and MAC387 may be helpful in the diagnosis of MSCP.
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication.