Article Text

Statistics from Altmetric.com
DESCRIPTION
We present two cases of subclavian steel syndrome to give an impression of the wide spectrum of possible symptoms and of the commonly used imaging modalities in subclavian steal syndrome.
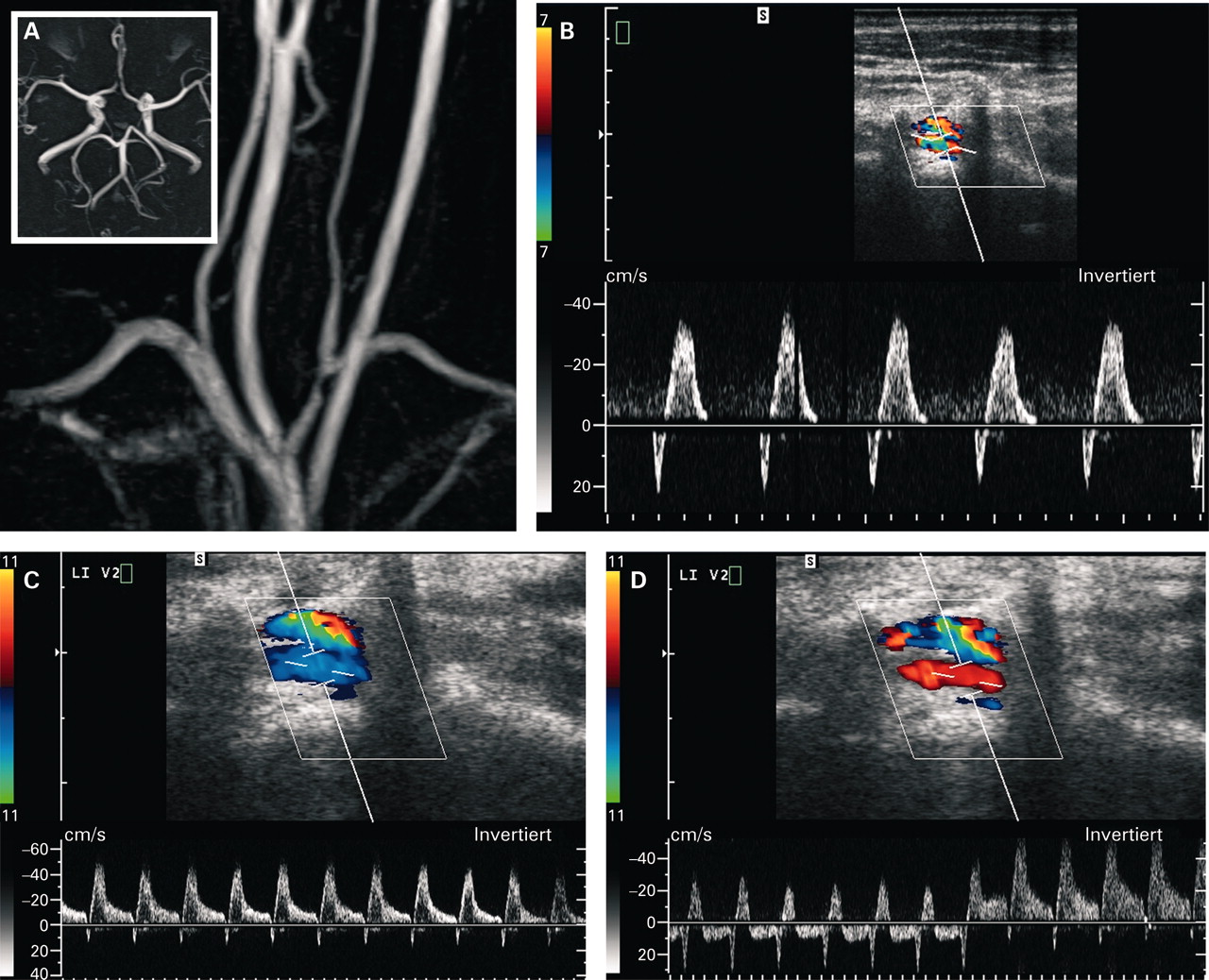
Case one is a 49-year-old female with periodic numbness in her left arm, followed by dizziness and nausea, occurring only while hanging laundry. MRI with angiography (fig 1A) and conventional angiography revealed a moderate proximal left subclavian artery stenosis (fig 2A–C), while Duplex ultrasound demonstrated the functional haemodynamic consequences (fig 1B–D) and the stenosis was eventually treated with a stenting procedure (fig 2D).

(A) Contrast-enhanced MRI/angiography of the supra-aortal arteries showing moderate left subclavian artery stenosis and unremarkable finding on time-of-flight MR-angiography of the intracranial vessels. (B) Doppler and duplex Doppler sonography showing a bidirectional wave-form with initial antegrade flow and subsequent retrograde flow in the V2 segment of the left vertebral artery. (C) Retrograde flow was increased at manual work and (D) was markedly increased after release of a pressure cuff on the left arm.

(A) Digital subtraction angiography showing moderate stenosis of the left subclavian artery; however, with dilatation at the origin of the left vertebral artery, (B) retrograde and weak contrast filling of the left vertebral artery also into the cervical segments in the later phase (C). (D) Blood flow was significantly increased after left subclavian artery stenting.
Case two is a 59-year-old male with chronic renal failure on haemodialysis presenting with acute left homonymous haemianopsia. His installed Cimino fistula was found enormously enlarged with calculated volume of total fistula flow 3945 ml/min. MRI of the brain demonstrated an acute ischaemic stroke of the occipital lobe (fig 3A, B). Further investigations showed a patent vertebrobasilar system, no subclavian artery stenosis and were negative for an embolic source (fig 3C, D). Ultrasonography of the brachiocephalic fistula revealed high haemodynamic demand (fig 4).1 Thus, the patient either suffered haemodynamic infarcts in two endbranches of the posterior cerebral artery or the oscillatory flow within the left vertebral artery caused clot formation leading to local embolic events.

MRI of the brain showing hyperintense lesions of the occipital lobe on fluid-attenuated inversion recovery (FLAIR) (A, arrows) and diffusion weighted imaging (DWI) (B, arrows) sequences; MR-angiography (C) showing patent subclavian, basilar and vertebral arteries, but abnormal flow in the left V4 segment (D, arrow).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Colour duplex sonography indicated retrograde flow in the V1 segment with vertebral vein running parallel to the artery. The Doppler spectrum showed a short orthograde flow with flow reversal and high negative flow in end diastolic. (B) Flow oscillation in the V3 segment with diminishment of the orthograde component in the Doppler spectrum. (C) Complete flow reversal (in red) in the left V4 segment with normal flow in the right V4 segment (in blue). (D) Colour duplex sonography of the brachial artery with high flow and spectral broadening. The calculated flow volume was 3945 ml/min. (E) Compression of the arteriovenous fistula caused cessation of retrograde flow and increase of the orthograde flow in the V1 segment (white arrow). (F) Compression of the arteriovenous fistula ended retrograde flow in the left V4 segment; however, orthograde flow could not be detected.
While CT angiography and MR angiography both are suitable for detecting a subclavian artery stenosis,2,3 both techniques are less suitable for detecting dynamic and subtle changes in blood flow. However, cranial CT and MRI can provide more information about acute or chronic ischaemic events in the vertebrobasilar territory. Conventional angiography can determine the degree of a stenosis with greatest accuracy and demonstrate retrograde flow.
Ultrasound investigation disclosed important haemodynamic aspects of the disease that were not observed by MR angiography.
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication.