Article Text

Statistics from Altmetric.com
DESCRIPTION
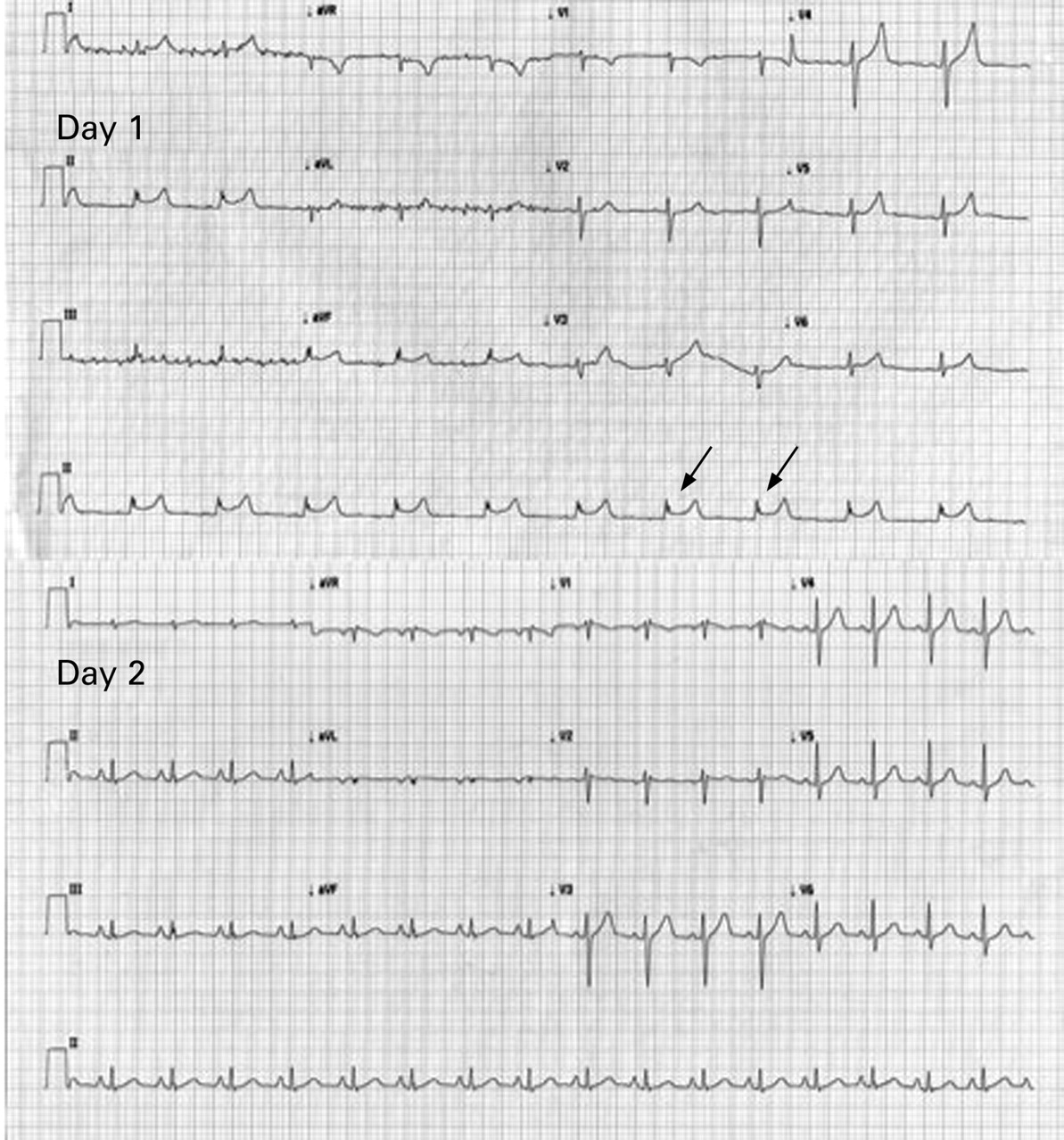
A 25-year-old male smoker with a history of depressive symptoms was brought to our emergency department in stuporous condition. He had allegedly ingested 720 mg of baclofen and about 30 mg of alprazolam in an attempt to commit suicide. Upon arrival in the unit (day 1), he was comatose with absent brain stem reflexes, mechanically ventilated, hypothermic with an oral temperature of 34.2°C (93.56° F) and hypotensive. A 12-lead electrocardiogram (ECG) showed regular sinus rhythm with a rate of 64 bpm, normal QRS, a QTc of 411 ms and intermittent Mobitz type II heart block. Osborn waves like J-point deflections secondary to hypothermia were identified most prominently in lead II (fig 1). Patient’s vitals and sensorium normalised over the next 24 h with supportive measures. A repeat 12-lead ECG on day 2 showed the disappearance of Osborn waves (figs 1 and 2).
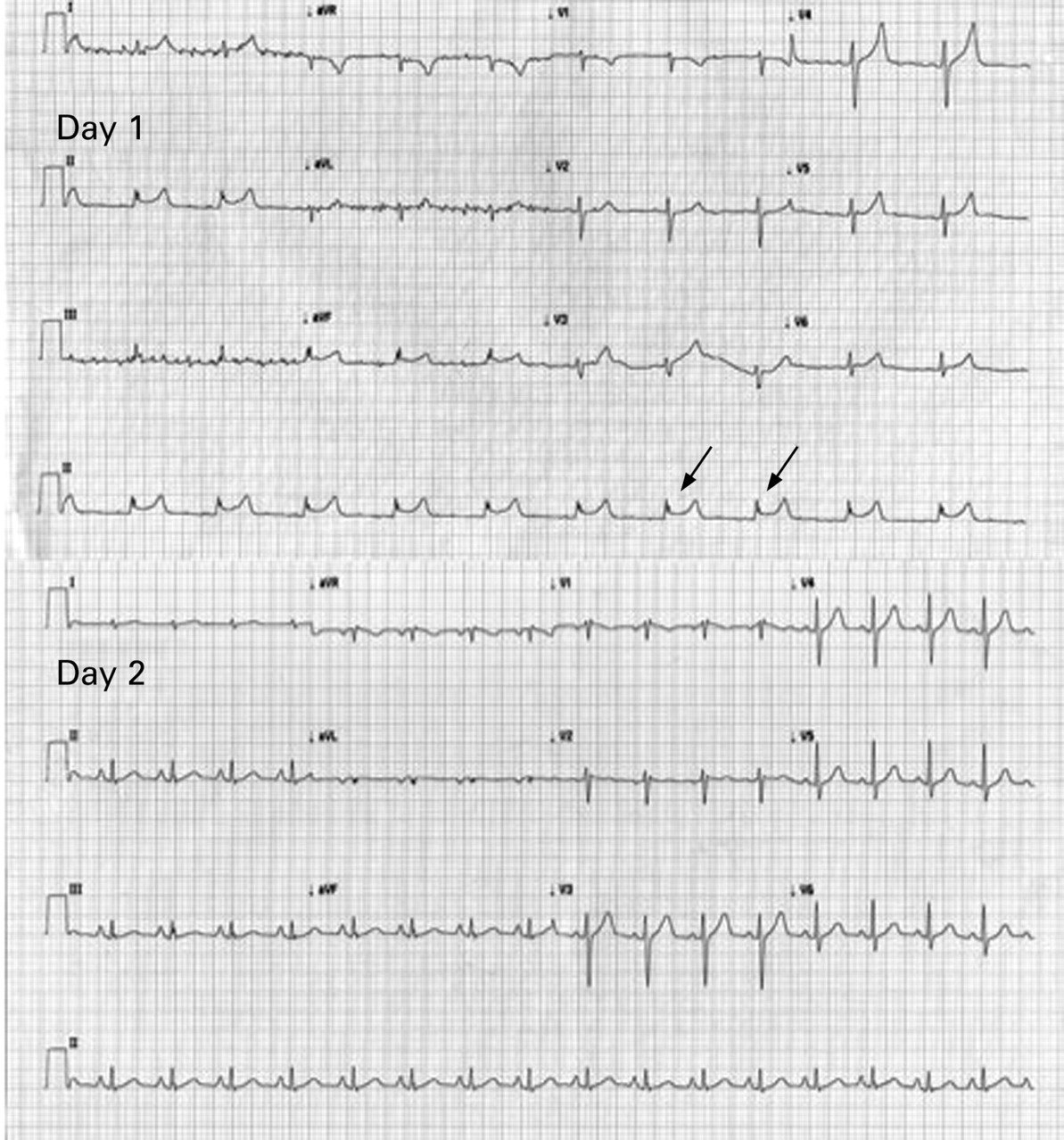
Resting 12-lead ECG tracing showing J-point deflection on day 1 that disappeared by day 2 with normalisation of temperature.

{kind=link}
{kind=link}
A close-up of the Osborn waves in lead II.
J point wave was first described by Tomaszewski in 19381 but named after JJ Osborn (1953) who reported2 systemic descriptions from his work in animal models of experimental hypothermia. It is classically defined as a dome or hump-shaped deflection seen at the R-ST junction (J point) and is also known as “camel-hump sign”, “late delta wave”, “hathook junction”, “hypothermic wave”, “J point wave”, “K wave” or “H wave”. It is most commonly described in hypothermia but can also be seen in hypercalcaemia, subarachnoid haemorrhage, cardiopulmonary arrest from oversedation and vasospatic angina among other.3 The wave is thought to be an ECG manifestation of increased ventricular transmural voltage gradient that is possible in many of these conditions.3 The waves regress with rewarming and are considered by many experts to be of arrhythmogenic potential.
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication.