Article Text

Summary
Aerosols are commonplace in the home and in industry as they provide a quick and controlled way of distributing chemicals or perfumes. It is well known that deliberating concentrating and inhaling vapours may result in dizziness, euphoria, blackouts, respiratory distress, cardiac and renal failure. However, in the most part, warnings and guidance on use are sparse. Here, a proven case of acute respiratory distress is presented and a reporting mechanism via the UK National Poisons Information Service (NPIS) directly from the Emergency Department (ED) is highlighted. In this case, as a result of our reporting, the aerosol was redesigned and redeployed as a trigger spray with better consumer guidance. Clinicians are reminded of the central role of the ED in the reporting of such hazards.
Statistics from Altmetric.com
BACKGROUND
Doctors are very aware of reporting adverse drug reactions using the “yellow card” system in the British National Formulary. But, for other chemicals, especially those in the occupational or consumer setting, we would like to inform front-line clinicians of the importance of reporting back to the UK National Poisons Information Service (NPIS) as a way of ensuring that adverse reactions are followed up by the UK Health and Safety Executive (HSE).
CASE PRESENTATION
A 40-year-old customer care manager attended a 2-h indoor demonstration of an upholstery cleaning product with eight other people. She was normally fit and well, not known to have any allergies, but smoked 20 cigarettes per day. Approximately 1 h after the demonstration, she began to develop a headache, sore eyes, a non-productive cough and feel progressively short of breath.
On presentation to the Emergency Department (ED), she was unable to speak in full sentences, had a respiratory rate of 44 breaths/min and oxygen saturations of 88% on air improving to 99% with a fraction of inspired oxygen (FiO2) of 0.6. We could not measure peak expiratory flow rate. There was reduced air entry throughout the chest with scattered wheeze in the mid and upper zones. Her pulse rate was 80/min, blood pressure was 122/62 mm Hg and she was afebrile.
INVESTIGATIONS
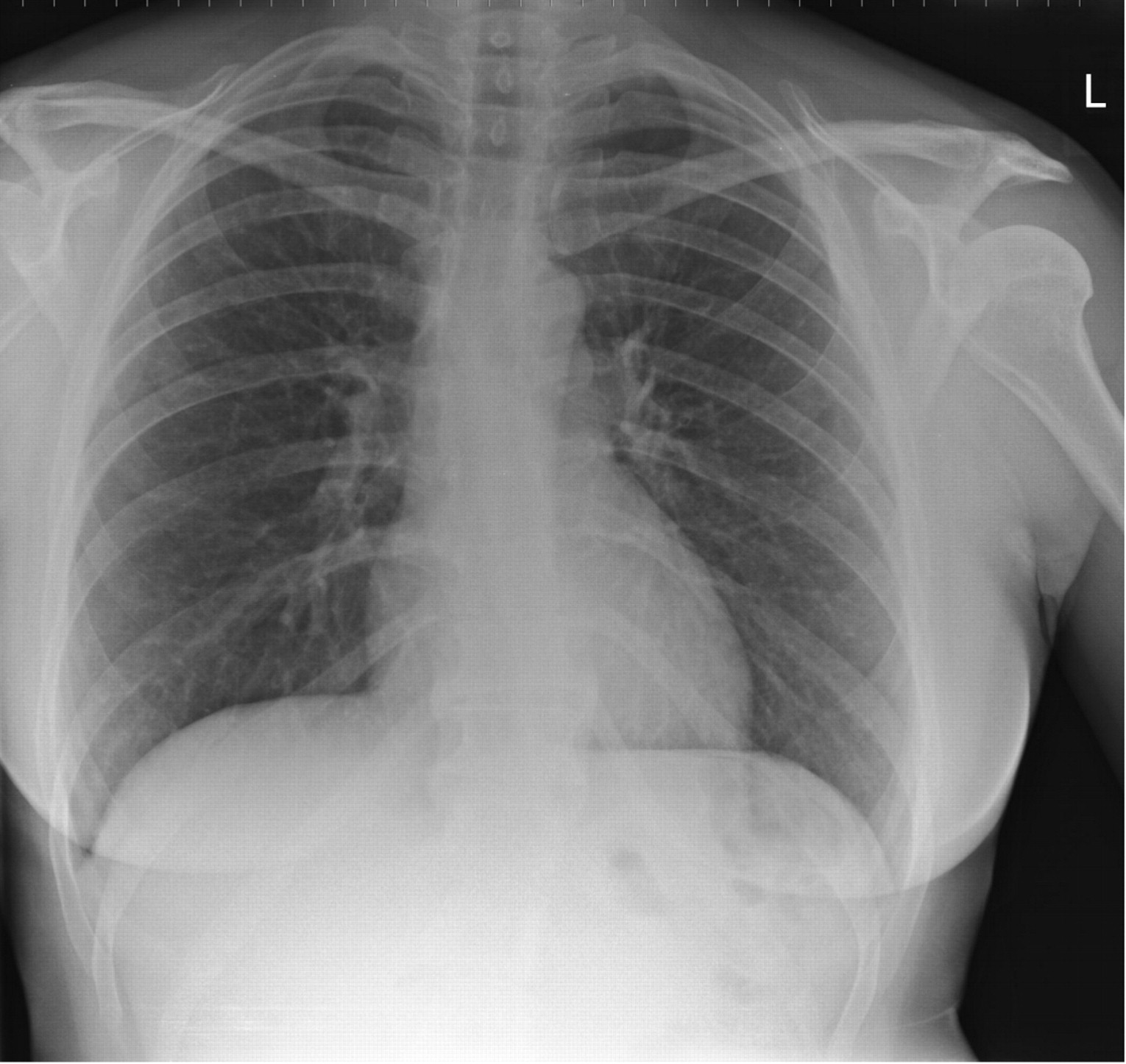
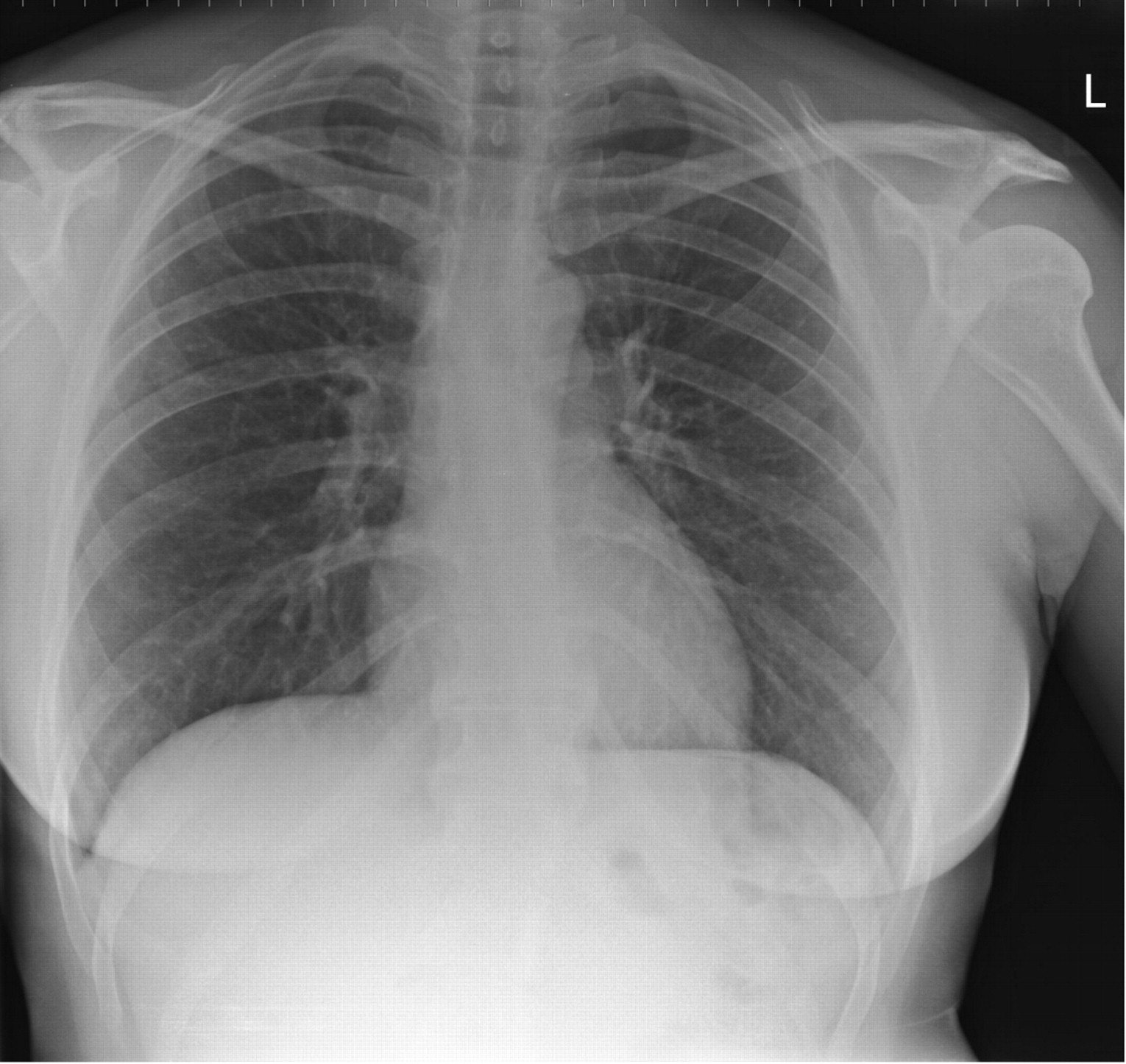
Full blood count revealed a mild neutrophilia of 11.8×109/litre (total white count 13.0×109/litre) and initial chest radiograph showed bilateral perihilar opacities with upper lobe diversion (fig 1). The 12-lead ECG was normal.

Anterior–posterior (AP) chest radiograph on admission showing bilateral perihilar opacification and upper lobe diversion.
DIFFERENTIAL DIAGNOSIS
We contacted the NPIS who pulled up the manufacturer’s safety data sheet for the cleaning product, which listed the chemical composition as: isobutane (1% to 5%), butane (5% to 10%), propane (10% to 30%) and naphtha hydrotreated light (30% to 60%). A diagnosis of probable hypersensitivity pneumonitis to one of the chemical constituents was made.
TREATMENT
In the emergency department the patient was treated with intravenous hydrocortisone, nebulised salbutamol and monitored oxygen therapy and admitted under the care of the medical team. After 24 h, the patient did not require any further supplemental oxygen therapy and was discharged with 5 days of oral prednisolone.
OUTCOME AND FOLLOW-UP
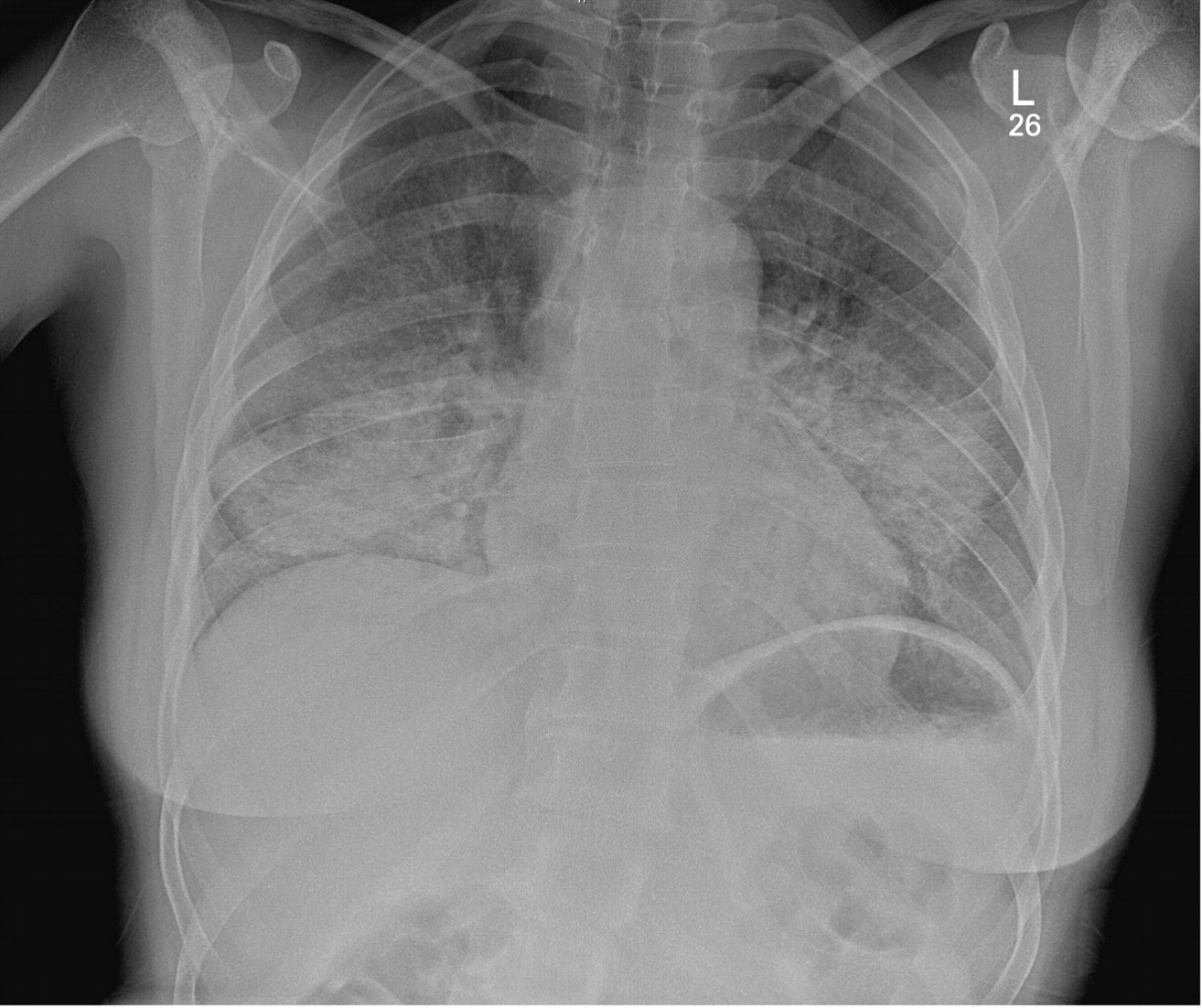
A repeat chest radiograph at 2 weeks post exposure was entirely normal and the patient was discharged from the respiratory clinic without complication or any further investigation (fig 2).
{kind=link}
{kind=link}
Posterior–anterior (PA) chest radiograph 2 weeks after exposure showing complete resolution.
DISCUSSION
Acute respiratory illnesses after exposure to noxious chemicals are seen frequently in the Emergency Department. Clinically, presentation can range from chest tightness and mild wheeze to full-blown adult respiratory distress syndrome (ARDS). In most cases, it is difficult to place a definite diagnosis and these patients are mostly managed on the severity of their presenting symptoms and response to simple therapy. In general, few minor cases are followed up after being treated unless they represent to the ED.
The severity of the symptoms in this case, coupled with the low dose exposure in a susceptible individual, led us to believe that this was probably a case of hypersensitivity pneumonitis (HP). HP is a group of immunologically mediated lung diseases provoked by a wide range of antigens ranging from organic particles to low molecular weight chemicals. Definite diagnosis relies on demonstrating bronchial hypersensitivity to a specific antigen and by excluding similar non-allergic inflammatory reactions such as toxic alveolitis and organic dust syndrome.1 Unfortunately, there is no single test that can make a diagnosis of HP in the ED.
We performed a literature search of the chemical constituents listed for the upholstery cleaner and noted that there were no reported instances of butane, isobutane or propane causing hypersensitivity pneumonitis or adult respiratory distress syndrome in people. However, the chief constituent, naphtha, is reported to cause a similar but pathologically distinct lung disease called chemical pneumonitis which, can be caused by inhalation or even ingestion of large amounts of naphtha.2 While chemical pneumonitis remained a possible diagnosis, the fact that only one of eight people equally exposed to the product strongly suggested an atopic origin, and so the diagnosis of hypersensitivity pneumonitis more likely.
In terms of treatment in the ED, we saw marked resolution of clinical symptoms upon the administration of intravenous and oral steroids. HP can be treated in the acute phase with steroids and there is good evidence in literature to support this. However, steroids are not recommended in the long-term treatment of HP as this may exacerbate the problem.3 The key to treating HP is to avoid the precipitating antigen; and we advised our patient to discontinue use of the upholstery cleaner and avoid all contact.
We examined the canister of the upholstery cleaner and noted a small text warning advising that the product should be used in a “well ventilated area”. From the packaging, it was not clear what level of ventilation was required to use the product safely. The aerosol product in question came in two forms: one to be used by consumers and the other as a specialist treatment for use by trained professionals. We followed the case up and contacted the manufacturer directly for their response to the adverse reaction. Cases of adverse reaction due to occupational exposure that are reported to the NPIS are obliged to be followed up by the HSE. Following the HSE’s advice, a working party was set up to modify the commercially available preparation. The manufacturer redesigned the product packaging so that prominent “blue mask” respiratory hazard symbols were conspicuously placed on the canister sides as well as a break through seal. A new guidance booklet was produced specifying respiratory protective equipment including a minimum filter size. The formulation of the product was also changed. The suspected allergen naphtha was removed from the formulation and replaced with propan-2-ol. An odour was also incorporated to increase awareness of product concentration in the environment and the delivery method was changed from a fine mist aerosol to a larger droplet trigger spray reducing the chances of deep bronchial inhalation.
LEARNING POINTS
Acute respiratory distress is not an uncommon presentation to the Emergency Department.
Treatment is usually supportive with bronchodilators and steroids.
The UK National Poisons Information Service (NPIS) remains an important reporting mechanism as well as a treatment resource.
Clinicians are encouraged to report directly to the manufacturers while maintaining patient confidentiality.
Even “single” adverse events can result in large changes.
Footnotes
Competing interests: None.
Patient consent: Patient/guardian consent was obtained for publication.