Article Text

Summary
An 87-year-old woman was admitted to our hospital with sepsis and foetid vaginal discharge. She presented an abdominal mass that had been present for the last 20 years, refused diagnostic or therapeutic procedures. A computed tomography scan detected a uterine body with multiple calcifications and an internal collection of 10 cm. No other infectious sources were apparent. A tentative diagnostic of pyometra was made and empiric antibiotic treatment was initiated. A hysteroscopy was performed with incomplete drainage of purulent material, due to important vaginal atrophy. In both blood and vaginal fluid cultures Prevotella spp. was isolated. Clinical evolution was favourable with metronidazole. The patient refused a hysterectomy or other surgical drainages, and she was discharged from hospital with oral antibiotics. The patient underwent antibiotic therapy during 1 month; 1 week after finishing this treatment, the patient died. The characteristics of clinical evolution in these last days were not known.
Statistics from Altmetric.com
BACKGROUND
Pyometra is an infrequent entity, characterised by an accumulation of pus in the uterine cavity. It mainly appears in postmenopausal women, usually associated to malignant entities of the genital tract. The main complications of pyometra are bacteraemia and sepsis as well as the feared spontaneous uterine perforation with secondary generalised peritonitis.1,2
CASE PRESENTATION
An 87-year-old woman was admitted to our hospital with a clinical history including fever, foetid grey vaginal discharge and a confusional state that had developed over the previous week. Twenty years ago, she noticed an infra-umbilical abdominal mass, but she did not accept any medical evaluation and thus no diagnosis was reached. There are no other medical or surgical antecedents of interest. A physical examination revealed a poorly active woman with a palpable mass in her lower abdomen. The mass was painful but muscular rigidity was absent and intestinal sounds were normal. Leucocytosis with neutrophilia and elevated serum concentration of C-reactive protein were detected. The rest of the haematological, biochemical and coagulation studies were normal. A simple abdominal x-ray showed a lower abdominal mass with multiple calcifications (fig 1). An ultrasonography revealed a heterogeneous mass, with a liquid collection inside of it. A computed tomography (CT) scan detected a large calcified myoma, with an intrauterine heterogeneous liquid collection over 10 cm in diameter (figs 2 and 3), suggestive of pyometra. Blood cultures were taken and empirical treatment with piperacillin/tazobactam was started. A gynaecology consultation was required. Carrying out a hysteroscopy was difficult because of the intense vaginal atrophy; putrid pus, draining throughout the uterine cervix, was observed and a sample was cultured. The patient refused hysterectomy or vaginal or abdominal drainage with anaesthesia.

Abdominal x-ray showing a calcified mass in the lower abdomen.

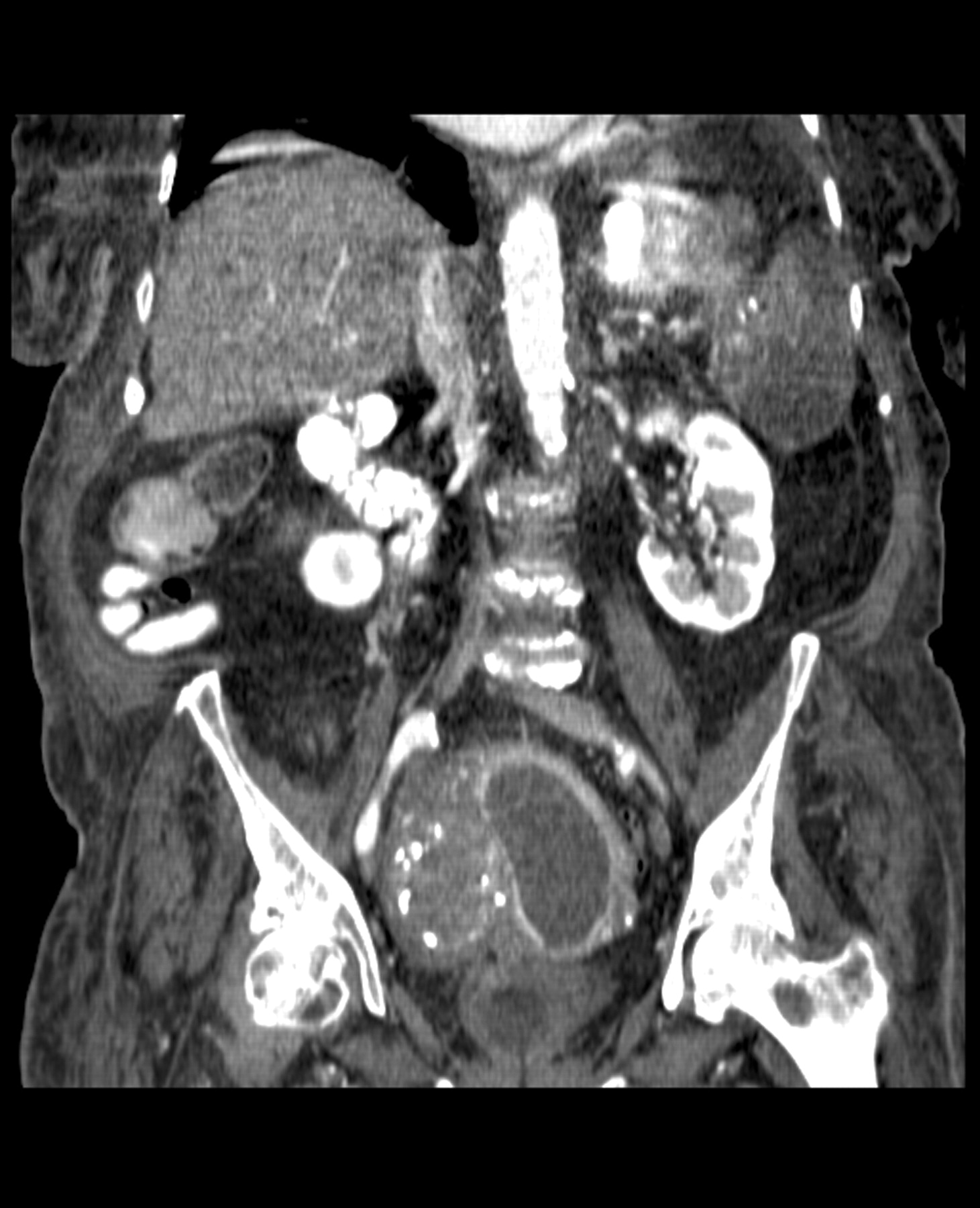
Computed tomography scan—coronal.

{kind=link}
{kind=link}
{kind=link}
Computed tomography scan—axial. A large calcified myoma, with an intrauterine heterogeneous liquid collection of about 10 cm in diameter without an air–fluid level; pneumoperitoneum is absent.
OUTCOME AND FOLLOW-UP
Prevotella spp. was isolated from both blood and uterine pus cultures. Intravenous metronidazole was initiated. The clinical course was favourable and she was asymptomatic 5 days later. The patient was discharged and prolonged oral metronidazole was indicated. We contacted the family by telephone 2 months later and they told us that the patient had carried out antibiotic therapy for 1 month; 1 week after finishing this treatment, the patient died. Clinical characteristics of this last period were not known.
DISCUSSION
Pyometra is an accumulation of pus in the uterine cavity. It represents 0.01–0.5% of gynaecological admissions, although the incidence increases to 13.6% in the elderly.3 Pyometra is predominantly diagnosed in postmenopausal women, usually associated with malignant lesions of the genital tract or radiotherapy treatment; predisposing benign idiopathic lesions have been described in some cases.4,5 The most frequent aetiological agents are Escherichia coli and Bacteroides fragilis, which are usually as mixed infections.6
When pyometra is diagnosed without complications, 50% of patients are asymptomatic and the rest show non-specific symptoms. CT scan shows a large uterus with an internal liquid collection, with or without an air–fluid level.
The patient in our case presented with an abdominal mass, which was probably a leiomyoma based on radiological characteristics and time evolution (20 years of evolution). Most likely, the growth of the mass had caused a serious drainage problem in the uterine cavity with posterior infection by anaerobes.
The main complications of pyometra are sepsis and the feared, although fortunately infrequent, spontaneous perforation with secondary peritonitis. In a literature review, only 22 cases of spontaneous rupture of pyometra have been described in the last decade, with a mortality of 30%; in this case the symptoms become severe and an acute abdomen often develops. In the evolution of the patient in our case, the spontaneous rupture of pyometra can not be excluded; effectively, in the 22 above-mentioned cases, pneumoperitoneum was detected by image techniques in only 47.4% and generalised peritonitis was absent in 53%.6
Spontaneous perforation of pyometra should be kept in mind as one of the differential diagnoses in elderly women with an acute abdomen, particularly if any gynaecological obstructing disease is present. Antibiotic therapy combined with total hysterectomy (or alternatively, in non-operable patients, cervix dilatation and cavity drainage) are the preferred treatments.6–8
LEARNING POINTS
Pyometra is an entity, characterised by the accumulation of pus in the uterine cavity, which is generally associated with causes that produce interference in the natural drainage of the uterine cavity.
The diagnosis can be carried out by CT, which shows a large uterus with an internal liquid collection, with or without an air–fluid level.
The main complications of pyometra are sepsis and spontaneous perforation with secondary peritonitis.
Footnotes
Competing interests: none.
Patient consent: Patient/guardian consent was obtained for publication.